Sistemas de Informação em Saúde para MunicÃpios - Secretaria de ...
Sistemas de Informação em Saúde para MunicÃpios - Secretaria de ...
Sistemas de Informação em Saúde para MunicÃpios - Secretaria de ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
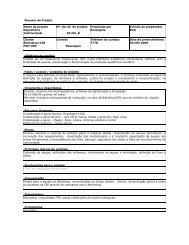
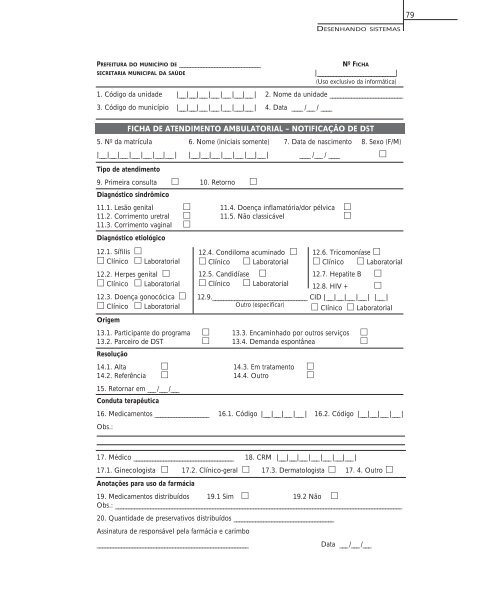
79DESENHANDO SISTEMASPREFEITURA DO MUNICÍPIO DE ______________________________SECRETARIA MUNICIPAL DA SAÚDENº FICHA|_____________________________|(Uso exclusivo da informática)1. Código da unida<strong>de</strong> |___ |___ |___ |___ |___ |___|___ | 2. Nome da unida<strong>de</strong> ___________________________3. Código do município |___ |___ |___ |___ |___ |___|___ | 4. Data ____ /___ / ____FICHA DE ATENDIMENTO AMBULATORIAL – NOTIFICAÇÃO DE DST5. Nº da matrícula 6. Nome (iniciais somente) 7. Data <strong>de</strong> nascimento 8. Sexo (F/M)|___ |___ |___ |___ |___ |___|___ | |___ |___ |___ |___ |___ |___|___ | ____ /___ / ____ Tipo <strong>de</strong> atendimento9. Primeira consulta 10. Retorno Diagnóstico sindrômico11.1. Lesão genital 11.4. Doença inflamatória/dor pélvica 11.2. Corrimento uretral 11.5. Não classicável 11.3. Corrimento vaginal Diagnóstico etiológico12.1. Sífilis Clínico Laboratorial12.2. Herpes genital Clínico Laboratorial12.3. Doença gonocócica Clínico LaboratorialOrig<strong>em</strong>12.4. Condiloma acuminado Clínico Laboratorial12.5. Candidíase Clínico Laboratorial12.6. Tricomoníase Clínico Laboratorial12.7. Hepatite B 12.8. HIV + 13.1. Participante do programa 13.3. Encaminhado por outros serviços 13.2. Parceiro <strong>de</strong> DST 13.4. D<strong>em</strong>anda espontânea Resolução12.9.___________________________________ CID |___ |___ |___ |___ | |___ |Outro (especificar) Clínico Laboratorial14.1. Alta 14.3. Em tratamento 14.2. Referência 14.4. Outro 15. Retornar <strong>em</strong> ___ /___ /___Conduta terapêutica16. Medicamentos ____________________ 16.1. Código |___ |___ |___ |___ | 16.2. Código |___ |___ |___ |___ |Obs.:17. Médico _____________________________________ 18. CRM |___ |___ |___ |___ |___ |___|___ |17.1. Ginecologista 17.2. Clínico-geral 17.3. Dermatologista 17. 4. Outro Anotações <strong>para</strong> uso da farmácia19. Medicamentos distribuídos 19.1 Sim 19.2 Não Obs.: __________________________________________________________________________________________________________20. Quantida<strong>de</strong> <strong>de</strong> preservativos distribuídos _____________________________________Assinatura <strong>de</strong> responsável pela farmácia e carimbo________________________________________________________Data ___ /___ /___