

Implementing food-based dietary guidelines for - United Nations ...
Implementing food-based dietary guidelines for - United Nations ...
Implementing food-based dietary guidelines for - United Nations ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
S40<br />
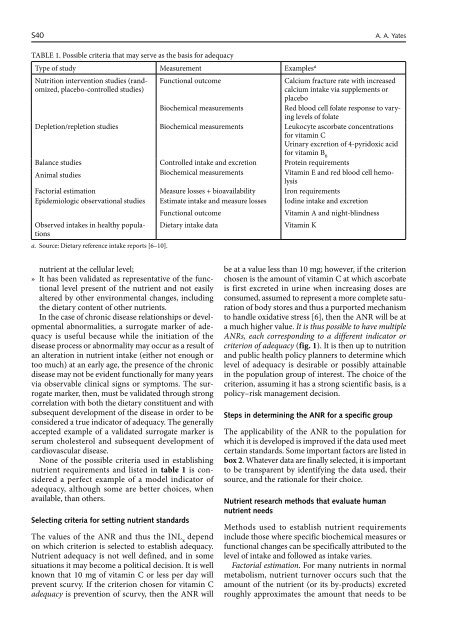
TABLE 1. Possible criteria that may serve as the basis <strong>for</strong> adequacy<br />
Type of study Measurement Examples a<br />
Nutrition intervention studies (randomized,<br />
placebo-controlled studies)<br />
nutrient at the cellular level;<br />
» It has been validated as representative of the functional<br />
level present of the nutrient and not easily<br />
altered by other environmental changes, including<br />
the <strong>dietary</strong> content of other nutrients.<br />
In the case of chronic disease relationships or developmental<br />
abnormalities, a surrogate marker of adequacy<br />
is useful because while the initiation of the<br />
disease process or abnormality may occur as a result of<br />
an alteration in nutrient intake (either not enough or<br />
too much) at an early age, the presence of the chronic<br />
disease may not be evident functionally <strong>for</strong> many years<br />
via observable clinical signs or symptoms. The surrogate<br />
marker, then, must be validated through strong<br />
correlation with both the <strong>dietary</strong> constituent and with<br />
subsequent development of the disease in order to be<br />
considered a true indicator of adequacy. The generally<br />
accepted example of a validated surrogate marker is<br />
serum cholesterol and subsequent development of<br />
cardiovascular disease.<br />
None of the possible criteria used in establishing<br />
nutrient requirements and listed in table 1 is considered<br />
a perfect example of a model indicator of<br />
adequacy, although some are better choices, when<br />
available, than others.<br />
Selecting criteria <strong>for</strong> setting nutrient standards<br />
The values of the ANR and thus the INL x depend<br />
on which criterion is selected to establish adequacy.<br />
Nutrient adequacy is not well defined, and in some<br />
situations it may become a political decision. It is well<br />
known that 10 mg of vitamin C or less per day will<br />
prevent scurvy. If the criterion chosen <strong>for</strong> vitamin C<br />
adequacy is prevention of scurvy, then the ANR will<br />
Functional outcome Calcium fracture rate with increased<br />
calcium intake via supplements or<br />
placebo<br />
Biochemical measurements Red blood cell folate response to varying<br />
levels of folate<br />
Depletion/repletion studies Biochemical measurements Leukocyte ascorbate concentrations<br />
<strong>for</strong> vitamin C<br />
Urinary excretion of 4-pyridoxic acid<br />
<strong>for</strong> vitamin B 6<br />
Balance studies Controlled intake and excretion Protein requirements<br />
Animal studies Biochemical measurements Vitamin E and red blood cell hemolysis<br />
Factorial estimation Measure losses + bioavailability Iron requirements<br />
Epidemiologic observational studies Estimate intake and measure losses Iodine intake and excretion<br />
Observed intakes in healthy populations<br />
a. Source: Dietary reference intake reports [6–10].<br />
Functional outcome Vitamin A and night-blindness<br />
Dietary intake data Vitamin K<br />
be at a value less than 10 mg; however, if the criterion<br />
chosen is the amount of vitamin C at which ascorbate<br />
is first excreted in urine when increasing doses are<br />
consumed, assumed to represent a more complete saturation<br />
of body stores and thus a purported mechanism<br />
to handle oxidative stress [6], then the ANR will be at<br />
a much higher value. It is thus possible to have multiple<br />
ANRs, each corresponding to a different indicator or<br />
criterion of adequacy (fig. 1). It is then up to nutrition<br />
and public health policy planners to determine which<br />
level of adequacy is desirable or possibly attainable<br />
in the population group of interest. The choice of the<br />
criterion, assuming it has a strong scientific basis, is a<br />
policy–risk management decision.<br />
Steps in determining the ANR <strong>for</strong> a specific group<br />
The applicability of the ANR to the population <strong>for</strong><br />
which it is developed is improved if the data used meet<br />
certain standards. Some important factors are listed in<br />
box 2. Whatever data are finally selected, it is important<br />
to be transparent by identifying the data used, their<br />
source, and the rationale <strong>for</strong> their choice.<br />
Nutrient research methods that evaluate human<br />
nutrient needs<br />
A. A. Yates<br />
Methods used to establish nutrient requirements<br />
include those where specific biochemical measures or<br />
functional changes can be specifically attributed to the<br />
level of intake and followed as intake varies.<br />
Factorial estimation. For many nutrients in normal<br />
metabolism, nutrient turnover occurs such that the<br />
amount of the nutrient (or its by-products) excreted<br />
roughly approximates the amount that needs to be

