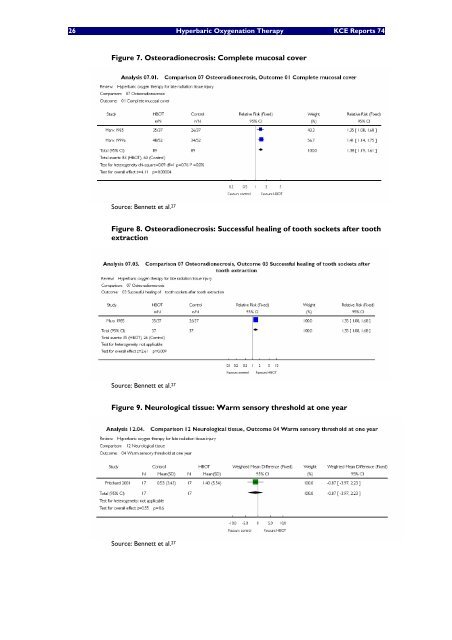
26 Hyperbaric Oxygenation Therapy <strong>KCE</strong> Reports 74 Figure 7. Osteoradionecrosis: Complete mucosal cover Source: Bennett et al. 27 Figure 8. Osteoradionecrosis: Successful healing of tooth sockets after tooth extraction Source: Bennett et al. 27 Figure 9. Neurological tissue: Warm sensory threshold at one year Source: Bennett et al. 27
<strong>KCE</strong> Reports 74 Hyperbaric Oxygenation Therapy 27 The HAS and the IECS assessments, 37, 38 and also the MSAC 2003 report come to similar conclusions as to the availability of evidence. 54 In a letter to the editor, 17 it was reported that a final self-assessment questionnaire administered to participants of one of the studies included in the Cochrane review found that also after 6-7 years no treatment effects seem to have been missed. 55 Within the COST B14 program (see before), a European RCT for adjunctive HBOT in osteo-integration in irradiated patients to prevent implant failures (study co-ordinator: C. Granstrom, Stockholm, Sweden) is reported to have started in October 2001, and another one on the role of HBOT in the treatment of late irradiation sequelae in the pelvic region (study co-ordinator: A. Van der Kleij, Amsterdam, The Netherlands) was reported to be in preparation in 2005. 42 However, no results have been found. 3.4.7 Delayed wound healing 3.4.7.1 Short description of the condition Problems wounds are a significant problem and are common in an ageing population. The most common are lower extremity ulcers, comprising venous ulcers, pressure ulcers and diabetic ulcers. In the US, foot ulcers in patients with diabetes are reported to contribute to over half of lower extremity amputations in a group at risk representing only 3% of the population. 8 Normal wound healing is normally a sequence of contamination and infection control, the resolution of inflammation and the regeneration of tissue. This normal wound healing process requires oxygen. Delayed wound healing and chronic wounds occur when this normal process is disturbed, and the healing rate of wounds has been shown to be oxygen dependent, by measurement of local oxygen tension in the vicinity of the wound. 8 Although wounds are, by nature, hypoxic the oxygen tensions from surrounding tissue is normally adequate to support normal healing of wounds. 3.4.7.2 Summary of the evidence Delayed wound healing in selected indications are accepted as indication for HBOT by both ECHM as UHMS. Those indications are mainly in diabetic patients with reduced peripheral perfusion, but also in arteriosclerotic patients in case of chronic critical ischemia (defined as periodical pain persistent at rest and needing regular analgesic treatment for more than two weeks, or ulceration or gangrene of foot and toes with low ankle systolic pressure). 8, 9 Those two indications are for the ECHM type 2, level B recommendations. 9 In addition HBOT is accepted for selected non-healing wounds caused by inflammatory processes (ECHM type 3, level C recommendation). 9 Both organisations stress the importance of transcutaneous oxygen pressure measurements (PtcO2) under hyperbaric conditions, since they provide a direct and quantitative assessment of the availability of oxygen around the wound. 8 Moreover, it can be used to assess the progression of wound healing after a series of HBOT treatments. There is abundant laboratory, animal study and physiological evidence to support the claims for HBOT to be effective in supporting wound healing. Clinical evidence is also available, mainly for the indication diabetic foot. The pathophysiology of diabetic foot ulceration involves a progressive neuropathy, leading to the deficiency of protective sensation and alterations in blood flow to the skin. In addition, diabetic patients have a greater tendency to develop peripheral artery disease. 8 Added to this the impaired immune response to infection, all these elements lead to ulceration problems that can lead to chronic wounds and eventually amputations. A Cochrane review from 2004 assessed the evidence for HBOT in chronic wounds. 32 This review pooled results from five trials. Four out of these were devoted to diabetic foot ulcers (with 147 patients in total). The authors calculated that the number needed to treat (NNT) with adjuvant HBOT to prevent one major amputation in the short term would be four. However, two of those trials were not blinded, leaving opportunity for biased decision making in supporting therapeutic decisions and assessments, while only one of the blinded trials report the outcome major amputation. This blinded but very small trial (n=18) showed no effect of adjunctive HBOT on major amputations (see Figure 11).