Benefit Reference Guide - The School District of Palm Beach County
Benefit Reference Guide - The School District of Palm Beach County
Benefit Reference Guide - The School District of Palm Beach County

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Dental<br />
Specialty Services for Managed Care Plan<br />
(S500PB and S700)<br />
• <strong>The</strong> fees within this overview <strong>of</strong> services apply when such<br />
services are performed by a participating general dentist, unless<br />
otherwise authorized by UnitedHealthcare Dental.*<br />
• If services are not listed within the Schedule <strong>of</strong> <strong>Benefit</strong>s and are<br />
performed by a participating general dentist, fees will be charged<br />
at the dentist’s usual and customary fee less 25%.<br />
• <strong>The</strong> participating general dentist you select may not perform all<br />
outlined procedures. <strong>The</strong> co-payments shown apply to general<br />
dentists who perform these procedures. <strong>The</strong>refore, you are<br />
encouraged to secure availability <strong>of</strong> the scheduled services with<br />
your participating general dentist.<br />
• Should the services <strong>of</strong> a specialist (Oral Surgeon, Endodontist,<br />
Orthodontist, Periodontist, Prosthodontist or Pedodontist) be<br />
necessary, you may receive this care in one <strong>of</strong> two ways: (1)<br />
You may go directly to a participating specialist with no referral<br />
and receive a 25% reduction <strong>of</strong>f the provider’s usual and<br />
customary fee; or (2) You may obtain prior written authorization<br />
by UnitedHealthcare Dental* and receive specialty treatment by<br />
an approved participating specialist at the listed co-payments.<br />
Please refer to the Specialty Care Referral Policy in your member<br />
ID packet.<br />
* UnitedHealthcare Dental plans are administered by Dental <strong>Benefit</strong> Providers, Inc.<br />
Managed Care Plans (S500PB and S700)<br />
Features:<br />
About fillings<br />
<strong>The</strong> aforementioned UnitedHealthcare Dental managed care<br />
programs provide coverage for the following fillings benefits:<br />
Amalgam (silver fillings) (S500PB and S700)<br />
• No co-payments - Covered 100%<br />
• Verify that your treating dentist provides amalgam fillings. If your<br />
dentist does not <strong>of</strong>fer amalgam fillings, you will receive a resin<br />
(white filling) and you will be responsible for the following copayments:<br />
Composite Resin (white fillings)<br />
S500PB<br />
• Anterior Teeth – Co-payment will apply from $25 - $105<br />
• Posterior Teeth – Co-payment will apply from $55 - $105<br />
S700<br />
• Anterior Teeth – Co-payment will apply from $30 - $115<br />
• Posterior Teeth – Co-payment will apply from $65 - $115<br />
Please discuss your treatment plan with your dentist prior to the<br />
initiation <strong>of</strong> treatment. If the dentist you selected does not cover the<br />
treatment you desire, please check with another dentist within our<br />
network. With this plan, you have the ability to select any dentist<br />
within the network at any time.<br />
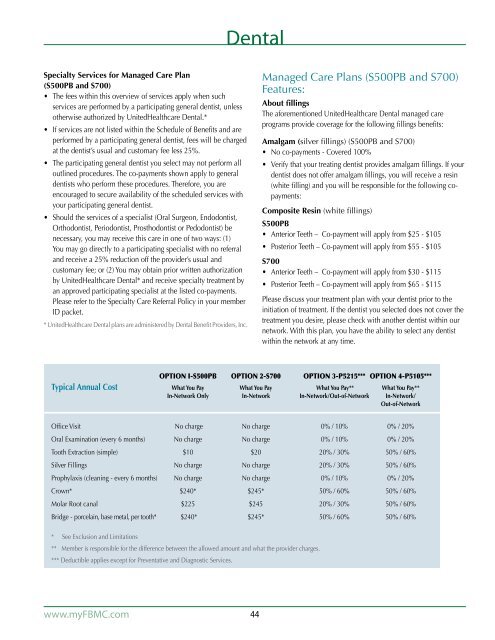
Option I-S500PB Option 2-S700 Option 3-P5215*** Option 4-P5105***<br />
Typical Annual Cost What You Pay What You Pay What You Pay** What You Pay**<br />
In-Network Only In-Network In-Network/Out-<strong>of</strong>-Network In-Network/<br />
Out-<strong>of</strong>-Network<br />
Office Visit No charge No charge 0% / 10% 0% / 20%<br />
Oral Examination (every 6 months) No charge No charge 0% / 10% 0% / 20%<br />
Tooth Extraction (simple) $10 $20 20% / 30% 50% / 60%<br />
Silver Fillings No charge No charge 20% / 30% 50% / 60%<br />
Prophylaxis (cleaning - every 6 months) No charge No charge 0% / 10% 0% / 20%<br />
Crown* $240* $245* 50% / 60% 50% / 60%<br />
Molar Root canal $225 $245 20% / 30% 50% / 60%<br />
Bridge - porcelain, base metal, per tooth* $240* $245* 50% / 60% 50% / 60%<br />
* See Exclusion and Limitations<br />
** Member is responsible for the difference between the allowed amount and what the provider charges.<br />
*** Deductible applies except for Preventative and Diagnostic Services.<br />
www.myFBMC.com<br />
44