

Volume 11 Issue 1 (February) - Australasian Society for Ultrasound ...
Volume 11 Issue 1 (February) - Australasian Society for Ultrasound ...
Volume 11 Issue 1 (February) - Australasian Society for Ultrasound ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
ASUM <strong>Ultrasound</strong> Bulletin <strong>February</strong> 2008; <strong>11</strong> (1): 25–29<br />
DIAGNOSTIC ULTRASOUND<br />
Interventional ultrasound – general principles and<br />
applications in gastroenterology<br />
Torben Lorentzen 1 and Christian Nolsøe 2<br />
1<br />
Department of Gastroenterologic Surgery, Copenhagen University Hospital at Herlev, 2 Department of Radiology,<br />
Copenhagen University Hospital at Koege, Denmark.<br />
Correspondence to Torben Lorentzen. Email tlo@dadlnet.dk<br />
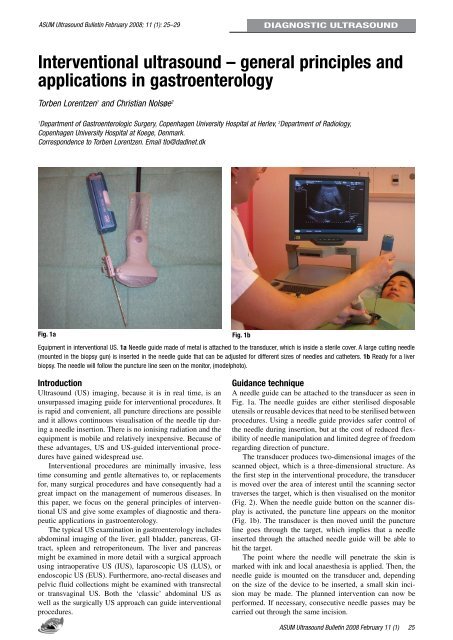
Fig. 1a<br />
Equipment in interventional US. 1a Needle guide made of metal is attached to the transducer, which is inside a sterile cover. A large cutting needle<br />
(mounted in the biopsy gun) is inserted in the needle guide that can be adjusted <strong>for</strong> different sizes of needles and catheters. 1b Ready <strong>for</strong> a liver<br />
biopsy. The needle will follow the puncture line seen on the monitor, (modelphoto).<br />
Fig. 1b<br />
Introduction<br />
<strong>Ultrasound</strong> (US) imaging, because it is in real time, is an<br />
unsurpassed imaging guide <strong>for</strong> interventional procedures. It<br />
is rapid and convenient, all puncture directions are possible<br />
and it allows continuous visualisation of the needle tip during<br />
a needle insertion. There is no ionising radiation and the<br />
equipment is mobile and relatively inexpensive. Because of<br />
these advantages, US and US-guided interventional procedures<br />
have gained widespread use.<br />
Interventional procedures are minimally invasive, less<br />
time consuming and gentle alternatives to, or replacements<br />
<strong>for</strong>, many surgical procedures and have consequently had a<br />
great impact on the management of numerous diseases. In<br />
this paper, we focus on the general principles of interventional<br />
US and give some examples of diagnostic and therapeutic<br />
applications in gastroenterology.<br />
The typical US examination in gastroenterology includes<br />
abdominal imaging of the liver, gall bladder, pancreas, GItract,<br />
spleen and retroperitoneum. The liver and pancreas<br />
might be examined in more detail with a surgical approach<br />
using intraoperative US (IUS), laparoscopic US (LUS), or<br />
endoscopic US (EUS). Furthermore, ano-rectal diseases and<br />
pelvic fluid collections might be examined with transrectal<br />
or transvaginal US. Both the ‘classic’ abdominal US as<br />
well as the surgically US approach can guide interventional<br />
procedures.<br />
Guidance technique<br />
A needle guide can be attached to the transducer as seen in<br />
Fig. 1a. The needle guides are either sterilised disposable<br />
utensils or reusable devices that need to be sterilised between<br />
procedures. Using a needle guide provides safer control of<br />
the needle during insertion, but at the cost of reduced flexibility<br />
of needle manipulation and limited degree of freedom<br />
regarding direction of puncture.<br />
The transducer produces two-dimensional images of the<br />
scanned object, which is a three-dimensional structure. As<br />
the first step in the interventional procedure, the transducer<br />
is moved over the area of interest until the scanning sector<br />
traverses the target, which is then visualised on the monitor<br />
(Fig. 2). When the needle guide button on the scanner display<br />
is activated, the puncture line appears on the monitor<br />
(Fig. 1b). The transducer is then moved until the puncture<br />
line goes through the target, which implies that a needle<br />
inserted through the attached needle guide will be able to<br />
hit the target.<br />
The point where the needle will penetrate the skin is<br />
marked with ink and local anaesthesia is applied. Then, the<br />
needle guide is mounted on the transducer and, depending<br />
on the size of the device to be inserted, a small skin incision<br />
may be made. The planned intervention can now be<br />
per<strong>for</strong>med. If necessary, consecutive needle passes may be<br />
carried out through the same incision.<br />
ASUM <strong>Ultrasound</strong> Bulletin 2008 <strong>February</strong> <strong>11</strong> (1)<br />
25














