

Volume 11 Issue 1 (February) - Australasian Society for Ultrasound ...
Volume 11 Issue 1 (February) - Australasian Society for Ultrasound ...
Volume 11 Issue 1 (February) - Australasian Society for Ultrasound ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
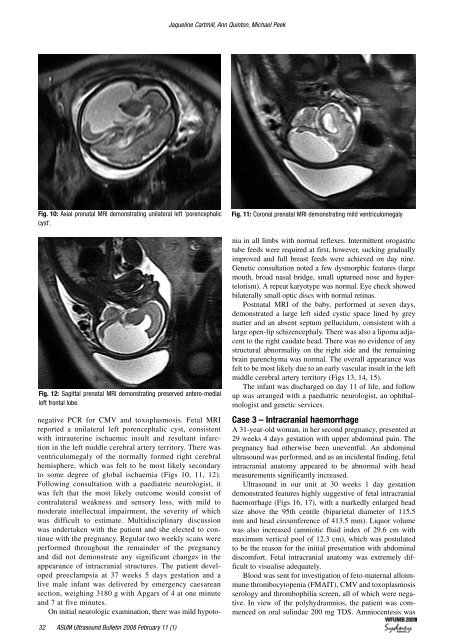
Jaqueline Cartmill, Ann Quinton, Michael Peek<br />
Fig. 10: Axial prenatal MRI demonstrating unilateral left 'porencephalic<br />
cyst'.<br />
Fig. 12: Sagittal prenatal MRI demonstrating preserved antero-medial<br />
left frontal lobe.<br />
Fig. <strong>11</strong>: Coronal prenatal MRI demonstrating mild ventriculomegaly<br />
negative PCR <strong>for</strong> CMV and toxoplasmosis. Fetal MRI<br />
reported a unilateral left porencephalic cyst, consistent<br />
with intrauterine ischaemic insult and resultant infarction<br />
in the left middle cerebral artery territory. There was<br />
ventriculomegaly of the normally <strong>for</strong>med right cerebral<br />
hemisphere, which was felt to be most likely secondary<br />
to some degree of global ischaemia (Figs 10, <strong>11</strong>, 12).<br />
Following consultation with a paediatric neurologist, it<br />
was felt that the most likely outcome would consist of<br />
contralateral weakness and sensory loss, with mild to<br />
moderate intellectual impairment, the severity of which<br />
was difficult to estimate. Multidisciplinary discussion<br />
was undertaken with the patient and she elected to continue<br />
with the pregnancy. Regular two weekly scans were<br />
per<strong>for</strong>med throughout the remainder of the pregnancy<br />
and did not demonstrate any significant changes in the<br />
appearance of intracranial structures. The patient developed<br />
preeclampsia at 37 weeks 5 days gestation and a<br />
live male infant was delivered by emergency caesarean<br />
section, weighing 3180 g with Apgars of 4 at one minute<br />
and 7 at five minutes.<br />
On initial neurologic examination, there was mild hypotonia<br />
in all limbs with normal reflexes. Intermittent orogastric<br />
tube feeds were required at first, however, sucking gradually<br />
improved and full breast feeds were achieved on day nine.<br />
Genetic consultation noted a few dysmorphic features (large<br />
mouth, broad nasal bridge, small upturned nose and hypertelorism).<br />
A repeat karyotype was normal. Eye check showed<br />
bilaterally small optic discs with normal retinas.<br />
Postnatal MRI of the baby, per<strong>for</strong>med at seven days,<br />
demonstrated a large left sided cystic space lined by grey<br />
matter and an absent septum pellucidum, consistent with a<br />
large open-lip schizencephaly. There was also a lipoma adjacent<br />
to the right caudate head. There was no evidence of any<br />
structural abnormality on the right side and the remaining<br />
brain parenchyma was normal. The overall appearance was<br />
felt to be most likely due to an early vascular insult in the left<br />
middle cerebral artery territory (Figs 13, 14, 15).<br />
The infant was discharged on day <strong>11</strong> of life, and follow<br />
up was arranged with a paediatric neurologist, an ophthalmologist<br />
and genetic services.<br />
Case 3 – Intracranial haemorrhage<br />
A 31-year-old woman, in her second pregnancy, presented at<br />
29 weeks 4 days gestation with upper abdominal pain. The<br />
pregnancy had otherwise been uneventful. An abdominal<br />
ultrasound was per<strong>for</strong>med, and as an incidental finding, fetal<br />
intracranial anatomy appeared to be abnormal with head<br />
measurements significantly increased.<br />
<strong>Ultrasound</strong> in our unit at 30 weeks 1 day gestation<br />
demonstrated features highly suggestive of fetal intracranial<br />
haemorrhage (Figs 16, 17), with a markedly enlarged head<br />
size above the 95th centile (biparietal diameter of <strong>11</strong>5.5<br />
mm and head circumference of 413.5 mm). Liquor volume<br />
was also increased (amniotic fluid index of 29.6 cm with<br />
maximum vertical pool of 12.3 cm), which was postulated<br />
to be the reason <strong>for</strong> the initial presentation with abdominal<br />
discom<strong>for</strong>t. Fetal intracranial anatomy was extremely difficult<br />
to visualise adequately.<br />
Blood was sent <strong>for</strong> investigation of feto-maternal alloimmune<br />
thrombocytopenia (FMAIT), CMV and toxoplasmosis<br />
serology and thrombophilia screen, all of which were negative.<br />
In view of the polyhydramnios, the patient was commenced<br />
on oral sulindac 200 mg TDS. Amniocentesis was<br />
2 ASUM <strong>Ultrasound</strong> Bulletin 2008 <strong>February</strong> <strong>11</strong> (1)














