

Vol 43 # 3 September 2011 - Kma.org.kw
Vol 43 # 3 September 2011 - Kma.org.kw
Vol 43 # 3 September 2011 - Kma.org.kw

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
214<br />
Combination of Ballistic Lithotripsy and Transurethral Plasmakinetic Resection ...<br />
<strong>September</strong> <strong>2011</strong><br />
Table 1: Clinical data before and after surgery<br />
Period<br />
IPSS<br />
(scores)<br />
QOL<br />
(scores)<br />
Qmax<br />
(ml/s)<br />
RUV<br />
(ml)<br />
Preoperative<br />
25.4 ± 4.1<br />
(17 - 34)<br />
4.2 ± 1.1<br />
(3 - 6)<br />
8.5 ± 4.2<br />
(4.3 - 14.2)<br />
78.6 ± 13.3<br />
(12 - 410)<br />
Postoperative<br />
5.5 ± 4.3*<br />
(0 - 13)<br />
1.3 ± 0.8*<br />
(0 - 2)<br />
23.1 ± 5.7*<br />
(17.2 - 27.1)<br />
17.2 ± 4.1*<br />
(0 - 26)<br />
* Statistically significant; p < 0.01<br />
anterograde resection, divided anterograde resection,<br />
divided retrograde enucleation and total retrograde<br />
enucleation of the prostate, respectively.<br />
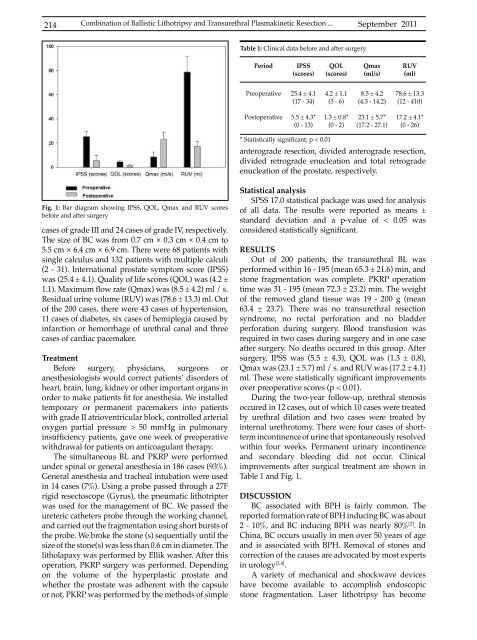
Fig. 1: Bar diagram showing IPSS, QOL, Qmax and RUV scores<br />
before and after surgery<br />
cases of grade III and 24 cases of grade IV, respectively.<br />
The size of BC was from 0.7 cm × 0.3 cm × 0.4 cm to<br />
5.5 cm × 6.4 cm × 6.9 cm. There were 68 patients with<br />
single calculus and 132 patients with multiple calculi<br />
(2 - 31). International prostate symptom score (IPSS)<br />
was (25.4 ± 4.1). Quality of life scores (QOL) was (4.2 ±<br />
1.1). Maximum flow rate (Qmax) was (8.5 ± 4.2) ml / s.<br />
Residual urine volume (RUV) was (78.6 ± 13.3) ml. Out<br />
of the 200 cases, there were <strong>43</strong> cases of hypertension,<br />
11 cases of diabetes, six cases of hemiplegia caused by<br />
infarction or hemorrhage of urethral canal and three<br />
cases of cardiac pacemaker.<br />
Treatment<br />
Before surgery, physicians, surgeons or<br />
anesthesiologists would correct patients’ disorders of<br />
heart, brain, lung, kidney or other important <strong>org</strong>ans in<br />
order to make patients fit for anesthesia. We installed<br />
temporary or permanent pacemakers into patients<br />
with grade II atrioventricular block, controlled arterial<br />
oxygen partial pressure > 50 mmHg in pulmonary<br />
insufficiency patients, gave one week of preoperative<br />
withdrawal for patients on anticoagulant therapy.<br />
The simultaneous BL and PKRP were performed<br />
under spinal or general anesthesia in 186 cases (93%).<br />
General anesthesia and tracheal intubation were used<br />
in 14 cases (7%). Using a probe passed through a 27F<br />
rigid resectoscope (Gyrus), the pneumatic lithotripter<br />
was used for the management of BC. We passed the<br />
ureteric catheters probe through the working channel,<br />
and carried out the fragmentation using short bursts of<br />
the probe. We broke the stone (s) sequentially until the<br />
size of the stone(s) was less than 0.6 cm in diameter. The<br />
litholapaxy was performed by Ellik washer. After this<br />
operation, PKRP surgery was performed. Depending<br />
on the volume of the hyperplastic prostate and<br />
whether the prostate was adherent with the capsule<br />
or not, PKRP was performed by the methods of simple<br />
Statistical analysis<br />
SPSS 17.0 statistical package was used for analysis<br />
of all data. The results were reported as means ±<br />
standard deviation and a p-value of < 0.05 was<br />
considered statistically significant.<br />
RESULTS<br />
Out of 200 patients, the transurethral BL was<br />
performed within 16 - 195 (mean 65.3 ± 21.6) min, and<br />
stone fragmentation was complete. PKRP operation<br />
time was 31 - 195 (mean 72.3 ± 23.2) min. The weight<br />
of the removed gland tissue was 19 - 200 g (mean<br />
63.4 ± 23.7). There was no transurethral resection<br />
syndrome, no rectal perforation and no bladder<br />
perforation during surgery. Blood transfusion was<br />
required in two cases during surgery and in one case<br />
after surgery. No deaths occured in this group. After<br />
surgery, IPSS was (5.5 ± 4.3), QOL was (1.3 ± 0.8),<br />
Qmax was (23.1 ± 5.7) ml / s. and RUV was (17.2 ± 4.1)<br />
ml. These were statistically significant improvements<br />
over preoperative scores (p < 0.01).<br />
During the two-year follow-up, urethral stenosis<br />
occured in 12 cases, out of which 10 cases were treated<br />
by urethral dilation and two cases were treated by<br />
internal urethrotomy. There were four cases of shortterm<br />
incontinence of urine that spontaneously resolved<br />
within four weeks. Permanent urinary incontinence<br />
and secondary bleeding did not occur. Clinical<br />
improvements after surgical treatment are shown in<br />
Table 1 and Fig. 1.<br />
DISCUSSION<br />
BC associated with BPH is fairly common. The<br />
reported formation rate of BPH inducing BC was about<br />
2 - 10%, and BC inducing BPH was nearly 80% [2] . In<br />
China, BC occurs usually in men over 50 years of age<br />
and is associated with BPH. Removal of stones and<br />
correction of the causes are advocated by most experts<br />
in urology [3,4] .<br />
A variety of mechanical and shoc<strong>kw</strong>ave devices<br />
have become available to accomplish endoscopic<br />
stone fragmentation. Laser lithotripsy has become













