PDO Medical examinations specification SP1230
PDO Medical examinations specification SP1230
PDO Medical examinations specification SP1230

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
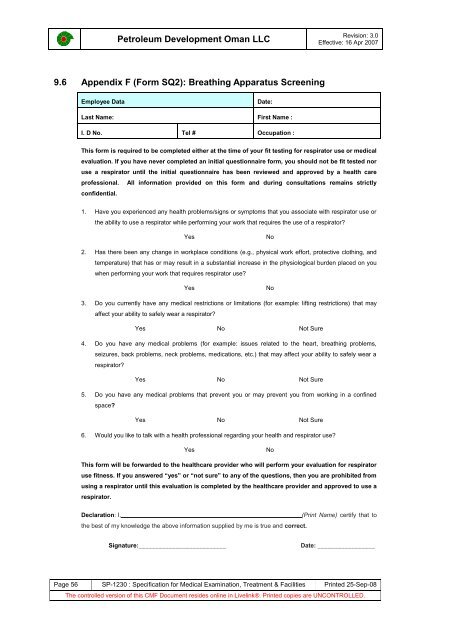
Petroleum Development Oman LLCRevision: 3.0Effective: 16 Apr 20079.6 Appendix F (Form SQ2): Breathing Apparatus ScreeningEmployee DataDate:Last Name: First Name :I. D No. Tel # Occupation :This form is required to be completed either at the time of your fit testing for respirator use or medicalevaluation. If you have never completed an initial questionnaire form, you should not be fit tested noruse a respirator until the initial questionnaire has been reviewed and approved by a health careprofessional. All information provided on this form and during consultations remains strictlyconfidential.1. Have you experienced any health problems/signs or symptoms that you associate with respirator use orthe ability to use a respirator while performing your work that requires the use of a respirator?YesNo2. Has there been any change in workplace conditions (e.g., physical work effort, protective clothing, andtemperature) that has or may result in a substantial increase in the physiological burden placed on youwhen performing your work that requires respirator use?YesNo3. Do you currently have any medical restrictions or limitations (for example: lifting restrictions) that mayaffect your ability to safely wear a respirator?Yes No Not Sure4. Do you have any medical problems (for example: issues related to the heart, breathing problems,seizures, back problems, neck problems, medications, etc.) that may affect your ability to safely wear arespirator?Yes No Not Sure5. Do you have any medical problems that prevent you or may prevent you from working in a confinedspace?Yes No Not Sure6. Would you like to talk with a health professional regarding your health and respirator use?YesNoThis form will be forwarded to the healthcare provider who will perform your evaluation for respiratoruse fitness. If you answered “yes” or “not sure” to any of the questions, then you are prohibited fromusing a respirator until this evaluation is completed by the healthcare provider and approved to use arespirator.Declaration: I, _______________________________ (Print Name) certify that tothe best of my knowledge the above information supplied by me is true and correct.Signature:__________________________Date: _________________Page 56 SP-1230 : Specification for <strong>Medical</strong> Examination, Treatment & Facilities Printed 25-Sep-08The controlled version of this CMF Document resides online in Livelink®. Printed copies are UNCONTROLLED.