Annex 12.1. Domestic abuseAnnex 12.1. Domestic abuseDomestic abuse: new and existing learning points from <strong>2006</strong> <strong>to</strong> <strong>2008</strong>This Enquiry continues <strong>to</strong> recommend that routine enquiry, ‘Asking the question’, should be made about domesticabuse, either when taking a social his<strong>to</strong>ry at booking or at another opportune point during a woman’s antenatalperiod. Midwives should give high priority <strong>to</strong> ‘Asking the question’ and <strong>to</strong> giving information <strong>to</strong> all women aboutdomestic abuse. The antenatal booking appointment may be the appropriate time <strong>to</strong> ‘ask the question’ or the midwifemay decide <strong>to</strong> delay until the following appointment when a relationship has already been established.All women should be seen alone at least once during the antenatal period <strong>to</strong> facilitate disclosure of domestic abuse.Any member of the maternity team who notices that a woman has an injury, for example a black eye, should asksympathetically, but directly, about how this occurred and be prepared <strong>to</strong> follow up this enquiry with information,advice and support as needed.The recent report Responding <strong>to</strong> Violence against Women and Children recommended, as does this Report, that healthservice providers and purchasers should have clear policies on the use of interpretation services that ensure thatwomen and children are able <strong>to</strong> disclose violence and abuse confidently and confidentially. 1When routine questioning is introduced, this must be accompanied by:• The establishment of an appropriate method of recording the response on the woman’s records, in such a way thatprotects her from further harm from the perpetra<strong>to</strong>r, if abuse is disclosed.• The development of local strategies for referral <strong>to</strong> a local multidisciplinary support network <strong>to</strong> which the woman canbe referred if necessary.Information about local sources of help and emergency help lines, such as those provided by Women’s Aid, should bedisplayed in suitable places in antenatal clinics, for example in the women’s <strong>to</strong>ilets, or printed as a routine at the bot<strong>to</strong>mof hand-held maternity notes or cooperation cards.Women who are known <strong>to</strong> suffer domestic abuse should not be regarded as ‘low risk’. They should be offered care thatinvolves other agencies and disciplines as needed for the individual’s situation, within a supportive environment. If theychoose midwifery-led care, the midwife should receive support and advice from an experienced colleague, for example theNamed Midwife for Safeguarding or a Supervisor of Midwives.It must be remembered that health professionals, <strong>to</strong>o, are victims of abuse and that domestic abuse occurs across allsocial classes and within all ethnic groups.BackgroundDomestic abuse has been the subject of separate chapters intwo previous Reports, 2,3 and readers are referred <strong>to</strong> them fora more detailed background information as well as the other,more recent, documents that are referenced in this Chapter.Domestic abuse has been defined as:Any incident of threatening behaviour or abuse (psychological,physical, sexual, financial or emotional) between adultswho are or have been intimate partners or family members,regardless of gender or sexuality. 4The term ‘domestic abuse’ is used in preference <strong>to</strong>‘domestic violence’ because the latter could be interpretedas relating <strong>to</strong> physical abuse alone. It also covers issues thatmainly concern women from minority ethnic backgrounds,such as forced marriage, female genital mutilation/cuttingand so-called ‘honour crimes’.Previous Reports have highlighted the issue of domesticabuse, and even murder, in pregnancy or after delivery. Asa result, a number of local and national initiatives wereintroduced, including sensitive routine questioning aboutexisting abuse during the antenatal period. One publication,Responding <strong>to</strong> Domestic Abuse, a Handbook for HealthProfessionals, 4 arose directly from these recommendations.The mothers affected by abuse: <strong>2006</strong>–08During the 3 years <strong>2006</strong>–08, 34 of the women who diedfrom any cause had features of domestic abuse. It is important<strong>to</strong> remember that although the perpetra<strong>to</strong>r is mos<strong>to</strong>ften the woman’s partner, it may also be other familymembers. This was the case for the majority of the 11women who were murdered, the abuse was fatal. Many of146 ª <strong>2011</strong> Centre for Maternal and Child Enquiries (CMACE), BJOG 118 (Suppl. 1), 1–203
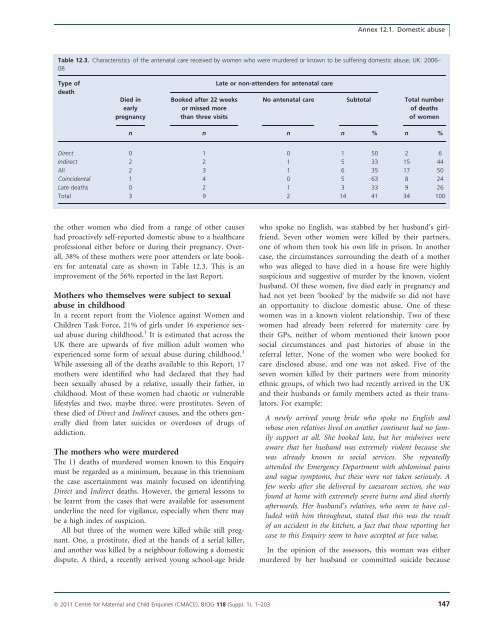
Annex 12.1. Domestic abuseTable 12.3. Characteristics of the antenatal care received by women who were murdered or known <strong>to</strong> be suffering domestic abuse; UK: <strong>2006</strong>–08Type ofdeathDied inearlypregnancyBooked after 22 weeksor missed morethan three visitsLate or non-attenders for antenatal careNo antenatal careSub<strong>to</strong>talTotal numberof <strong>deaths</strong>of womenn n n n % n %Direct 0 1 0 1 50 2 6Indirect 2 2 1 5 33 15 44All 2 3 1 6 35 17 50Coincidental 1 4 0 5 63 8 24Late <strong>deaths</strong> 0 2 1 3 33 9 26Total 3 9 2 14 41 34 100the other women who died from a range of other causeshad proactively self-reported domestic abuse <strong>to</strong> a healthcareprofessional either before or during their pregnancy. Overall,38% of these mothers were poor attenders or late bookersfor antenatal care as shown in Table 12.3. This is animprovement of the 56% reported in the last Report.<strong>Mothers</strong> who themselves were subject <strong>to</strong> sexualabuse in childhoodIn a recent report from the Violence against Women andChildren Task Force, 21% of girls under 16 experience sexualabuse during childhood. 1 It is estimated that across theUK there are upwards of five million adult women whoexperienced some form of sexual abuse during childhood. 1While assessing all of the <strong>deaths</strong> available <strong>to</strong> this Report, 17mothers were identified who had declared that they hadbeen sexually abused by a relative, usually their father, inchildhood. Most of these women had chaotic or vulnerablelifestyles and two, maybe three, were prostitutes. Seven ofthese died of Direct and Indirect causes, and the others generallydied from later suicides or overdoses of drugs ofaddiction.The mothers who were murderedThe 11 <strong>deaths</strong> of murdered women known <strong>to</strong> this Enquirymust be regarded as a minimum, because in this trienniumthe case ascertainment was mainly focused on identifyingDirect and Indirect <strong>deaths</strong>. However, the general lessons <strong>to</strong>be learnt from the cases that were available for assessmentunderline the need for vigilance, especially when there maybe a high index of suspicion.All but three of the women were killed while still pregnant.One, a prostitute, died at the hands of a serial killer,and another was killed by a neighbour following a domesticdispute. A third, a recently arrived young school-age bridewho spoke no English, was stabbed by her husband’s girlfriend.Seven other women were killed by their partners,one of whom then <strong>to</strong>ok his own life in prison. In anothercase, the circumstances surrounding the death of a motherwho was alleged <strong>to</strong> have died in a house fire were highlysuspicious and suggestive of murder by the known, violenthusband. Of these women, five died early in pregnancy andhad not yet been ‘booked’ by the midwife so did not havean opportunity <strong>to</strong> disclose domestic abuse. One of thesewomen was in a known violent relationship. Two of thesewomen had already been referred for maternity care bytheir GPs, neither of whom mentioned their known poorsocial circumstances and past his<strong>to</strong>ries of abuse in thereferral letter. None of the women who were booked forcare disclosed abuse, and one was not asked. Five of theseven women killed by their partners were from minorityethnic groups, of which two had recently arrived in the UKand their husbands or family members acted as their transla<strong>to</strong>rs.For example:A newly arrived young bride who spoke no English andwhose own relatives lived on another continent had no familysupport at all. She booked late, but her midwives wereaware that her husband was extremely violent because shewas already known <strong>to</strong> social services. She repeatedlyattended the Emergency Department with abdominal painsand vague symp<strong>to</strong>ms, but these were not taken seriously. Afew weeks after she delivered by caesarean section, she wasfound at home with extremely severe burns and died shortlyafterwards. Her husband’s relatives, who seem <strong>to</strong> have colludedwith him throughout, stated that this was the resul<strong>to</strong>f an accident in the kitchen, a fact that those reporting hercase <strong>to</strong> this Enquiry seem <strong>to</strong> have accepted at face value.In the opinion of the assessors, this woman was eithermurdered by her husband or committed suicide becauseª <strong>2011</strong> Centre for Maternal and Child Enquiries (CMACE), BJOG 118 (Suppl. 1), 1–203 147
- Page 1:
Volume 118, Supplement 1, March 201
- Page 4 and 5:
AcknowledgementsSaving Mothers’ L
- Page 6 and 7:
AcknowledgementsAcknowledgementsCMA
- Page 8 and 9:
Forewordbeen written jointly by a m
- Page 10 and 11:
‘Top ten’ recommendationsServic
- Page 12 and 13:
‘Top ten’ recommendationscommun
- Page 14 and 15:
‘Top ten’ recommendationsof suc
- Page 16 and 17:
‘Top ten’ recommendationsMarch
- Page 18 and 19:
Oates et al.Back to basicsM Oates 1
- Page 20 and 21:
Oates et al.BreathlessnessBreathles
- Page 22 and 23:
Oates et al.appropriate pathway of
- Page 24 and 25:
LewisIntroduction: Aims, objectives
- Page 26 and 27:
LewisAn important limitation of ran
- Page 28 and 29:
Lewismaternal and public health-pol
- Page 30 and 31:
Lewisresult in a live birth at any
- Page 32 and 33:
LewisChapter 1: The women who died
- Page 34 and 35:
Lewiswho would not have been identi
- Page 36 and 37:
Lewis1098Rate per 100 000 materniti
- Page 38 and 39:
LewisTable 1.4. Numbers and rates o
- Page 40 and 41:
Lewis2.50Rate per 100 000 materniti
- Page 42 and 43:
LewisTable 1.9. Number of maternal
- Page 44 and 45:
LewisTable 1.12. Numbers and percen
- Page 46 and 47:
LewisThere were cases where a major
- Page 48 and 49:
LewisBox 1.5. Classifications of Bo
- Page 50 and 51:
LewisTable 1.20. Number and estimat
- Page 52 and 53:
LewisNew countries of the European
- Page 54 and 55:
LewisTable 1.23. Direct and Indirec
- Page 56 and 57:
LewisTable 1.26. Characteristics* o
- Page 58 and 59:
Lewis4 Lewis G (ed). The Confidenti
- Page 60 and 61:
DrifeTable 2.1. Direct deaths from
- Page 62 and 63:
Drifewomen who died in 2006-08 had
- Page 64 and 65:
Drifedelivery she became breathless
- Page 66 and 67:
DrifePathological overviewFourteen
- Page 68 and 69:
NeilsonChapter 3: Pre-eclampsia and
- Page 70 and 71:
Neilsontrue, and what might be the
- Page 72 and 73:
NeilsonConclusionThe number of deat
- Page 74 and 75:
NormanBackgroundIn the UK, major ob
- Page 76 and 77:
Normanwhich there was catastrophic
- Page 78 and 79:
Normanrecommendations made in succe
- Page 80 and 81:
DawsonBox 5.1. The UK amniotic flui
- Page 82 and 83:
Dawsontry despite an extensive sear
- Page 84 and 85:
O’HerlihyTable 6.1. Numbers of Di
- Page 86 and 87:
O’Herlihytoxic shock syndrome aft
- Page 88 and 89:
HarperGroup A b-haemolytic streptoc
- Page 90 and 91:
Harperthe 6-week postnatal period,
- Page 92 and 93:
Harpera major intrapartum haemorrha
- Page 94 and 95:
HarperBox 7.1. Signs and symptoms o
- Page 96 and 97:
Harperwoman was given several litre
- Page 98 and 99: Harper2 Lamagni TL, Efstratiou A, D
- Page 100 and 101: LucasTable A7.1 Proposed new catego
- Page 102 and 103: Lucasthe same infection scenario as
- Page 104 and 105: McClure, CooperChapter 8: Anaesthes
- Page 106 and 107: McClure, Cooperaddress, but protoco
- Page 108 and 109: McClure, CooperPostpartum haemorrha
- Page 110 and 111: McClure, CooperWorkloadA number of
- Page 112 and 113: Nelson-PiercyTable 9.1. Indirect ma
- Page 114 and 115: Nelson-Piercynary arteries. In view
- Page 116 and 117: Nelson-Piercynormal left ventricle
- Page 118 and 119: LucasAnnex 9.1. Pathological overvi
- Page 120 and 121: Lucasdiac death that is non-ischaem
- Page 122 and 123: de Swiet et al.causes but are aggra
- Page 124 and 125: de Swiet et al.died of SUDEP before
- Page 126 and 127: de Swiet et al.for 6 weeks after de
- Page 128 and 129: de Swiet et al.mised. The obstetric
- Page 130 and 131: de Swiet et al.CancerPregnancy does
- Page 132 and 133: de Swiet et al.a thorough autopsy w
- Page 134 and 135: Oates, CantwellChapter 11: Deaths f
- Page 136 and 137: Oates, CantwellTable 11.1. Timing o
- Page 138 and 139: Oates, CantwellTable 11.5. Maternal
- Page 140 and 141: Oates, CantwellChild protection iss
- Page 142 and 143: Oates, CantwellAll women who are su
- Page 144 and 145: Oates, Cantwell4 Kendel RE, Chalmer
- Page 146 and 147: Lewismaternal mortality rates or ra
- Page 150 and 151: Annex 12.1. Domestic abuseshe could
- Page 152 and 153: Garrod et al.supportive but challen
- Page 154 and 155: Garrod et al.• Culture and system
- Page 156 and 157: Garrod et al.the second stage and s
- Page 158 and 159: Garrod et al.through the still heal
- Page 160 and 161: ShakespeareChapter 14: General prac
- Page 162 and 163: Shakespeareemergency caesarean sect
- Page 164 and 165: ShakespeareCardiac diseaseDeaths fr
- Page 166 and 167: Shakespearereduce the risks to the
- Page 168 and 169: ShakespeareManaging a maternal deat
- Page 170 and 171: Hulbertin the ED was of a high qual
- Page 172 and 173: HulbertPre-eclampsia/eclampsia: lea
- Page 174 and 175: HulbertTransfersWhen the obstetric
- Page 176 and 177: Clutton-Brocksimply the case that s
- Page 178 and 179: Clutton-BrockDiagnosis of sepsisTak
- Page 180 and 181: Clutton-Brockpulseless electrical a
- Page 182 and 183: Clutton-BrockImprovement Scotland (
- Page 184 and 185: Lucas, Millward-Sadler95 mmHg. This
- Page 186 and 187: Lucas, Millward-Sadleran agreed mai
- Page 188 and 189: Annex 17.1. The main clinico-tholog
- Page 190 and 191: MillerAppendix 1: The method of Enq
- Page 192 and 193: MillerDatanotificationNotificationR
- Page 194 and 195: Knight• investigating different m
- Page 196 and 197: Knightbaseline incidence against wh
- Page 198 and 199:
LennoxAppendix 2B: Summary of Scott
- Page 200 and 201:
LennoxEvidence of effective managem
- Page 202 and 203:
Appendix 3: Contributors to the Mat
- Page 204 and 205:
Appendix 3: Contributors to the Mat