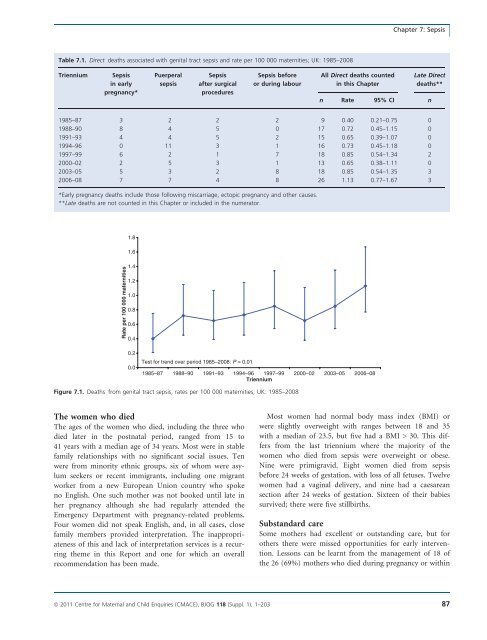
HarperGroup A b-haemolytic strep<strong>to</strong>coccus(Strep<strong>to</strong>coccus pyogenes): learningpointsThe number of <strong>maternal</strong> <strong>deaths</strong> from Group A b-haemolyticstrep<strong>to</strong>coccus (Strep<strong>to</strong>coccus pyogenes) infectionhas been increasing over the past 10 years.Group A strep<strong>to</strong>coccus is typically community basedand 5–30% of the population are asymp<strong>to</strong>matic carrierson skin or in throat. 1 It is easily spread by person-<strong>to</strong>personcontact or by droplet spread from a person withinfection.Strep<strong>to</strong>coccal sore throat is one of the most commonbacterial infections of childhood, and all of the motherswho died from Group A strep<strong>to</strong>coccal sepsis eitherworked with, or had, young children. Several mothersor family members had a his<strong>to</strong>ry of recent sore throa<strong>to</strong>r respira<strong>to</strong>ry infection.Contamination of the perineum is more likely when awoman or her family or close contacts have a sorethroat or upper respira<strong>to</strong>ry infection as the organismmay be transferred from the throat or nose via herhands <strong>to</strong> her perineum. Antenatal education shouldraise awareness of this and the importance of good personalhygiene and washing hands before and after usingthe lava<strong>to</strong>ry or changing sanitary <strong>to</strong>wels.IntroductionUnlike many other causes of direct <strong>maternal</strong> mortality,<strong>deaths</strong> from genital tract sepsis have risen rather thandeclined this triennium. Indeed, genital tract sepsis hasbecome the leading cause of Direct <strong>maternal</strong> death in theUK for the first time since these Confidential Enquiriesin<strong>to</strong> Maternal Deaths commenced in 1952. This is a causefor concern, particularly as it has occurred against a backgroundof an overall decrease in <strong>maternal</strong> mortality. But,as discussed in this Chapter, many of these <strong>deaths</strong> werefrom community-aquired Group A strep<strong>to</strong>coccal disease,mirroring an overall background increase in mortality fromthis disease in the general population. 2 For many of thesewomen, the outcome was unavoidable despite excellent carebecause of the rapid course and late presentation of the illness.However, in others, possible opportunities <strong>to</strong> savelives may have been missed and lessons remain <strong>to</strong> belearnt.Sepsis should never be underestimated. Its course isoften insidious and staff need <strong>to</strong> be aware that women withserious illness, especially sepsis, may appear deceptively wellbefore suddenly collapsing, often with little or no warning.Once established, sepsis may be fulminating and irreversiblewith rapid deterioration in<strong>to</strong> septic shock, disseminatedintravascular coagulation and multi-organ failure. The clinicalcourse is often so short, especially in Group A strep<strong>to</strong>coccalinfection, that by the time women present <strong>to</strong>hospital, it is <strong>to</strong>o late <strong>to</strong> save them. As a healthcare workersaid: ‘Even with modern medicine, an experienced team ofdoc<strong>to</strong>rs and midwives could not save a young pregnantwoman. The rapid deterioration caused by the overwhelmingsepsis, despite desperate attempts <strong>to</strong> resuscitate her, willnever be forgotten.’Sepsis is complex, incompletely unders<strong>to</strong>od, often difficult<strong>to</strong> recognise and manage, and presents a continuingchallenge. Some <strong>deaths</strong> will always be unavoidable, but bettertraining, a structured approach, good care in the community,and, in hospital, prompt investigation andtreatment, particularly immediate intravenous antibiotictreatment and early involvement of senior obstetricians, anaesthetistsand critical care consultants, may help in future<strong>to</strong> save some lives. Further information about the pathophysiology,clinical features and management of sepsis isgiven in Chapter 16 and should be read in conjunctionwith this chapter.Summary of key findings for <strong>2006</strong>–08The <strong>deaths</strong> of 29 women who died from genital tract sepsis,as traditionally defined by this Report, were reportedthis triennium. Of these, 26 Direct <strong>deaths</strong> are counted inthis Chapter and the remaining three, which were LateDirect <strong>deaths</strong> occurring more than 6 weeks after delivery,outside the international classification for <strong>maternal</strong> <strong>deaths</strong>,are counted in Chapter 12. One of these was also associatedwith haemorrhage. These three <strong>deaths</strong> are discussed herebecause the women concerned became ill before or soonafter delivery and they may contribute <strong>to</strong> the overall lessons<strong>to</strong> be learnt from these cases.The mortality rate from sepsis for this triennium, <strong>2006</strong>–08, is 1.13 (95% CI 0.77–1.67) per 100 000 maternities,compared with 0.85 (95% CI 0.54–1.35) for the last reportand the rate of 0.65 (95% CI 0.38–1.11) for 2000–02,although this increase has not reached statistical significance(P = 0.1). These rates are shown in Table 7.1 andFigure 7.1.The main reason for the rise in <strong>maternal</strong> mortalityfrom sepsis in this triennium is the increased number of<strong>deaths</strong> caused by community-acquired b-haemolytic strep<strong>to</strong>coccusLancefield Group A (Strep<strong>to</strong>coccus pyogenes).Most women had signs and symp<strong>to</strong>ms of severe sepsis bythe time they presented <strong>to</strong> hospital. Although there hasbeen much concern in recent years about hospitalacquiredinfection with ‘superbugs’, there is no evidenceof this apart from one woman who was already known <strong>to</strong>be a carrier.86 ª <strong>2011</strong> Centre for Maternal and Child Enquiries (CMACE), BJOG 118 (Suppl. 1), 1–203
Chapter 7: SepsisTable 7.1. Direct <strong>deaths</strong> associated with genital tract sepsis and rate per 100 000 maternities; UK: 1985–<strong>2008</strong>TrienniumSepsisin earlypregnancy*PuerperalsepsisSepsisafter surgicalproceduresSepsis beforeor during labourAll Direct <strong>deaths</strong> countedin this ChapterLate Direct<strong>deaths</strong>**n Rate 95% CI n1985–87 3 2 2 2 9 0.40 0.21–0.75 01988–90 8 4 5 0 17 0.72 0.45–1.15 01991–93 4 4 5 2 15 0.65 0.39–1.07 01994–96 0 11 3 1 16 0.73 0.45–1.18 01997–99 6 2 1 7 18 0.85 0.54–1.34 22000–02 2 5 3 1 13 0.65 0.38–1.11 02003–05 5 3 2 8 18 0.85 0.54–1.35 3<strong>2006</strong>–08 7 7 4 8 26 1.13 0.77–1.67 3*Early pregnancy <strong>deaths</strong> include those following miscarriage, ec<strong>to</strong>pic pregnancy and other causes.**Late <strong>deaths</strong> are not counted in this Chapter or included in the numera<strong>to</strong>r.Rate per 100 000 maternities1.81.61.41.21.00.80.60.40.20.0Test for trend over period 1985–<strong>2008</strong>: P = 0.011985–87 1988–90 1991–93 1994–96 1997–99 2000–02 2003–05 <strong>2006</strong>–08TrienniumFigure 7.1. Deaths from genital tract sepsis, rates per 100 000 maternities; UK: 1985–<strong>2008</strong>The women who diedThe ages of the women who died, including the three whodied later in the postnatal period, ranged from 15 <strong>to</strong>41 years with a median age of 34 years. Most were in stablefamily relationships with no significant social issues. Tenwere from minority ethnic groups, six of whom were asylumseekers or recent immigrants, including one migrantworker from a new European Union country who spokeno English. One such mother was not booked until late inher pregnancy although she had regularly attended theEmergency Department with pregnancy-related problems.Four women did not speak English, and, in all cases, closefamily members provided interpretation. The inappropriatenessof this and lack of interpretation services is a recurringtheme in this Report and one for which an overallrecommendation has been made.Most women had normal body mass index (BMI) orwere slightly overweight with ranges between 18 and 35with a median of 23.5, but five had a BMI > 30. This differsfrom the last triennium where the majority of thewomen who died from sepsis were overweight or obese.Nine were primigravid. Eight women died from sepsisbefore 24 weeks of gestation, with loss of all fetuses. Twelvewomen had a vaginal delivery, and nine had a caesareansection after 24 weeks of gestation. Sixteen of their babiessurvived; there were five stillbirths.Substandard careSome mothers had excellent or outstanding care, but forothers there were missed opportunities for early intervention.Lessons can be learnt from the management of 18 ofthe 26 (69%) mothers who died during pregnancy or withinª <strong>2011</strong> Centre for Maternal and Child Enquiries (CMACE), BJOG 118 (Suppl. 1), 1–203 87
- Page 1:
Volume 118, Supplement 1, March 201
- Page 4 and 5:
AcknowledgementsSaving Mothers’ L
- Page 6 and 7:
AcknowledgementsAcknowledgementsCMA
- Page 8 and 9:
Forewordbeen written jointly by a m
- Page 10 and 11:
‘Top ten’ recommendationsServic
- Page 12 and 13:
‘Top ten’ recommendationscommun
- Page 14 and 15:
‘Top ten’ recommendationsof suc
- Page 16 and 17:
‘Top ten’ recommendationsMarch
- Page 18 and 19:
Oates et al.Back to basicsM Oates 1
- Page 20 and 21:
Oates et al.BreathlessnessBreathles
- Page 22 and 23:
Oates et al.appropriate pathway of
- Page 24 and 25:
LewisIntroduction: Aims, objectives
- Page 26 and 27:
LewisAn important limitation of ran
- Page 28 and 29:
Lewismaternal and public health-pol
- Page 30 and 31:
Lewisresult in a live birth at any
- Page 32 and 33:
LewisChapter 1: The women who died
- Page 34 and 35:
Lewiswho would not have been identi
- Page 36 and 37:
Lewis1098Rate per 100 000 materniti
- Page 38 and 39: LewisTable 1.4. Numbers and rates o
- Page 40 and 41: Lewis2.50Rate per 100 000 materniti
- Page 42 and 43: LewisTable 1.9. Number of maternal
- Page 44 and 45: LewisTable 1.12. Numbers and percen
- Page 46 and 47: LewisThere were cases where a major
- Page 48 and 49: LewisBox 1.5. Classifications of Bo
- Page 50 and 51: LewisTable 1.20. Number and estimat
- Page 52 and 53: LewisNew countries of the European
- Page 54 and 55: LewisTable 1.23. Direct and Indirec
- Page 56 and 57: LewisTable 1.26. Characteristics* o
- Page 58 and 59: Lewis4 Lewis G (ed). The Confidenti
- Page 60 and 61: DrifeTable 2.1. Direct deaths from
- Page 62 and 63: Drifewomen who died in 2006-08 had
- Page 64 and 65: Drifedelivery she became breathless
- Page 66 and 67: DrifePathological overviewFourteen
- Page 68 and 69: NeilsonChapter 3: Pre-eclampsia and
- Page 70 and 71: Neilsontrue, and what might be the
- Page 72 and 73: NeilsonConclusionThe number of deat
- Page 74 and 75: NormanBackgroundIn the UK, major ob
- Page 76 and 77: Normanwhich there was catastrophic
- Page 78 and 79: Normanrecommendations made in succe
- Page 80 and 81: DawsonBox 5.1. The UK amniotic flui
- Page 82 and 83: Dawsontry despite an extensive sear
- Page 84 and 85: O’HerlihyTable 6.1. Numbers of Di
- Page 86 and 87: O’Herlihytoxic shock syndrome aft
- Page 90 and 91: Harperthe 6-week postnatal period,
- Page 92 and 93: Harpera major intrapartum haemorrha
- Page 94 and 95: HarperBox 7.1. Signs and symptoms o
- Page 96 and 97: Harperwoman was given several litre
- Page 98 and 99: Harper2 Lamagni TL, Efstratiou A, D
- Page 100 and 101: LucasTable A7.1 Proposed new catego
- Page 102 and 103: Lucasthe same infection scenario as
- Page 104 and 105: McClure, CooperChapter 8: Anaesthes
- Page 106 and 107: McClure, Cooperaddress, but protoco
- Page 108 and 109: McClure, CooperPostpartum haemorrha
- Page 110 and 111: McClure, CooperWorkloadA number of
- Page 112 and 113: Nelson-PiercyTable 9.1. Indirect ma
- Page 114 and 115: Nelson-Piercynary arteries. In view
- Page 116 and 117: Nelson-Piercynormal left ventricle
- Page 118 and 119: LucasAnnex 9.1. Pathological overvi
- Page 120 and 121: Lucasdiac death that is non-ischaem
- Page 122 and 123: de Swiet et al.causes but are aggra
- Page 124 and 125: de Swiet et al.died of SUDEP before
- Page 126 and 127: de Swiet et al.for 6 weeks after de
- Page 128 and 129: de Swiet et al.mised. The obstetric
- Page 130 and 131: de Swiet et al.CancerPregnancy does
- Page 132 and 133: de Swiet et al.a thorough autopsy w
- Page 134 and 135: Oates, CantwellChapter 11: Deaths f
- Page 136 and 137: Oates, CantwellTable 11.1. Timing o
- Page 138 and 139:
Oates, CantwellTable 11.5. Maternal
- Page 140 and 141:
Oates, CantwellChild protection iss
- Page 142 and 143:
Oates, CantwellAll women who are su
- Page 144 and 145:
Oates, Cantwell4 Kendel RE, Chalmer
- Page 146 and 147:
Lewismaternal mortality rates or ra
- Page 148 and 149:
Annex 12.1. Domestic abuseAnnex 12.
- Page 150 and 151:
Annex 12.1. Domestic abuseshe could
- Page 152 and 153:
Garrod et al.supportive but challen
- Page 154 and 155:
Garrod et al.• Culture and system
- Page 156 and 157:
Garrod et al.the second stage and s
- Page 158 and 159:
Garrod et al.through the still heal
- Page 160 and 161:
ShakespeareChapter 14: General prac
- Page 162 and 163:
Shakespeareemergency caesarean sect
- Page 164 and 165:
ShakespeareCardiac diseaseDeaths fr
- Page 166 and 167:
Shakespearereduce the risks to the
- Page 168 and 169:
ShakespeareManaging a maternal deat
- Page 170 and 171:
Hulbertin the ED was of a high qual
- Page 172 and 173:
HulbertPre-eclampsia/eclampsia: lea
- Page 174 and 175:
HulbertTransfersWhen the obstetric
- Page 176 and 177:
Clutton-Brocksimply the case that s
- Page 178 and 179:
Clutton-BrockDiagnosis of sepsisTak
- Page 180 and 181:
Clutton-Brockpulseless electrical a
- Page 182 and 183:
Clutton-BrockImprovement Scotland (
- Page 184 and 185:
Lucas, Millward-Sadler95 mmHg. This
- Page 186 and 187:
Lucas, Millward-Sadleran agreed mai
- Page 188 and 189:
Annex 17.1. The main clinico-tholog
- Page 190 and 191:
MillerAppendix 1: The method of Enq
- Page 192 and 193:
MillerDatanotificationNotificationR
- Page 194 and 195:
Knight• investigating different m
- Page 196 and 197:
Knightbaseline incidence against wh
- Page 198 and 199:
LennoxAppendix 2B: Summary of Scott
- Page 200 and 201:
LennoxEvidence of effective managem
- Page 202 and 203:
Appendix 3: Contributors to the Mat
- Page 204 and 205:
Appendix 3: Contributors to the Mat