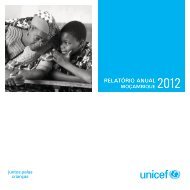
Mozambique National <strong>Human</strong> <strong>Development</strong> Report 2007Box 7.3The use of cotrimoxazole to preventHIV-related infections in AfricaUNAIDS and WHO recommend the use of cotrimoxazole in Africa for prophylaxisin adults and children living with HIV and AIDS, as part of a minimumpackage of treatment. Criteria for the use of the medication havealready been established, covering the selection of patients, the drug regimen,the duration of treatment, follow-up, the supply of the drug, educationand training, monitoring of drug resistance and adverse effects.Manuals for prophylaxis programmes have already been published.Cotrimoxazole costs between US$8 and US$17 per person per yearfor prophylaxis. It is widely available on the continent, and preliminaryanalyses have shown that the use of cotrimoxazole prophylaxis is a costefficientintervention in Africa, particularly when combined with growingaccess to voluntary counselling and testing for HIV infection.The generalised prophylactic or preventive use of cotrimoxazole inAfrica was postponed for a long time due to inconsistencies in the researchresults. Two studies held in Ivory Coast in 1999, one by French researchersand the other by American scientists, showed that the drug reduces the frequencyof opportunist diseases among HIV-positive people. One of thesestudies recorded a fall in the death rate from HIV-related diseases.Preliminary results from two studies sponsored by UNAIDS in SouthAfrica and Malawi confirmed that cotrimoxazole is safe in people withHIV, and the study in Malawi indicated significant beneficial impacts onmortality (WHO 2000).Common HIV-related infections in sub-Saharan Africa, which can beprevented by cotrimoxazole, include certain bacterial pneumonias anddiarrhoeal diseases. The fact that administering cotrimoxazole does notrequire medical staff with special training is an advantage, comparedwith ART.Graph 7.2National distribution of PLWHon ART by province, July 2005Niassa 2%C. Delgado 1%Nampula 2%Zambézia 4%Tete 8%Manica 5%Sofala 8%Inhambane 1%Gaza 4%Maputo P. 7%Maputo C. 58%Table 7.2Distribution of PLWA on ART bysex/age/province/district, to November 2006Province Number
National Strategies against the Spread and Impact of HIV and AIDSlogical criteria, the selected individuals shoulddemonstrate guarantees of compliance. They sign oragree verbally to an undertaking that they will complywith all the recommendations. To start the treatment,the protocol for including patients must bestrictly complied with, and the evaluation process atthe health units may last for approximately a month.This delays the onset of treatment, worsening stillfurther the state of the patient. (Survey on Adherenceto the ARS, MISAU/University of Columbia, 2004).There is a limit per health unit in the quotasattributed. The decision on who will benefit from thetreatment depends on the treatment managementcommittee operating in each health unit.But the greatest constraint is that most HIV-positivepeople do not know that they are HIV-positive.Those with access to the GATV mostly have initial difficultiesin accepting their condition, which compromisestimely guidance on the various possibilities ofpreventing the rapid evolution of the infection to thestate of illness.More than this, cultural factors, and particularlybelief in the possibility of cure through certain traditionalpractices impact negatively on the attitude andbehaviour of people towards the disease and its treatment.But above all, the lack of adequate informationis the main constraint in this sphere.Although there is little local factual informationabout the problems faced by the PLWA who arereceiving anti-retroviral treatment, a few studies, thatcannot be generalised, show that many peopleundergoing treatment keep it secret from their familyand even from their spouses (Survey on Adherenceto the ARS, ibid, 2004).Often this attitude makes it difficult to complycorrectly with the medication, namely taking thedrugs daily and at specific times, or abstaining fromalcohol. Those who work fear that their colleaguesmay find out that they are taking regular medication,and will discover that they are AIDS patients undergoingtreatment. This means that often they fail withthe medication. Stigma and discrimination are stillcommon in the workplace, and there are alsoreports of some patients being abandoned by theirfamilies.In the case of children, caregivers need to betrained to provide the drugs to them. Particularly theprovision of paediatric syrups to the youngest childrenrequires specific skills. Often, these caregiversare mothers or fathers who are infected with HIV andmight be weak or sick themselves, or elderly peoplewho might also be weak.A further important factor is diet. Taking thedrugs requires a regular and balanced diet. Most ofthe patients are very poor, with serious financialproblems, and often find themselves involuntarilycompelled to interrupt the treatment because ofhunger, since ingesting the drugs while fasting exacerbatesdiscomfort and weakness. There are someinitiatives to grant a basic basket of foodstuffs to peopleundergoing treatment, but these do not covereveryone.Undesirable side effects caused by the drugs areamong the factors that often influence temporaryinterruption of the medication, which is very serious,since it increases the risk of developing resistanceand of therapeutic failure.This expansion necessarily involves lifting thecommunity taboos about HIV infection and AIDS. Tocontrol AIDS, it must be accepted that it is a diseaselike many others, and that people living with HIV andAIDS are normal. Only by overcoming stigma, discriminationand fear can we improve the impact ofthe various interventions until we reach the lastwoman in the most remote parts of the country.Confidentiality, stigma and discriminationConfidentiality and the duty of maintaining patients’state of health private involve a compulsory internationalnorm of professional ethics. It is the duty of allhealth professionals to keep the diagnosis of thepatient secret, whatever it may be, while at the sametime it is the patient’s right to want, or not, his or herdirect relatives, or anybody else, to be informed ofhis or her state of health.Nowadays, because of AIDS, this concept isbecoming more complex. There is an urgent need todeal with human rights around the principles of confidentialityand privacy and the possible consequencesfor public health in responses against HIVand AIDS.Furthermore, for a campaign of HIV and AIDSprevention to be crowned with success, strategiesmust be defined to encourage people bearing the diseaseto break the silence. Up to now, a large proportionof the Mozambican population still sees AIDS,not as a problem for everybody, but only as somethingthat concerns other people, since many havenever seen an AIDS patient, although they exist nearthem and even in their own families.55