Peer Support Services12. Assistive tools, technologies, worksheets, etc. can be used by the Peer Support staff to work with the served individual to improve his/her communication abouttreatment, symptoms, improvements, etc. with treating behavioral health <strong>and</strong> medical practitioners.DocumentationRequirements1. Providers must document services in accordance with the specifications for documentation requirements specified in Part II, Section V <strong>of</strong> the Provider Manual.2. Each 15 minute unit <strong>of</strong> service provided must be documented within the individual’s medical record. Although there is no single prescribed format for documentation(a log may be used), the following elements MUST be included for every unit <strong>of</strong> service provided:a. the specific type <strong>of</strong> intervention must be documentedb. the date <strong>of</strong> service must be namedc. the number <strong>of</strong> unit(s) <strong>of</strong> service must be namedd. the practitioner level providing the service/unit must be namedFor example, a group led by a Practitioner Level 4 that lasts 1 hour should be documented as 4 units <strong>of</strong> H0038HQU4U6 <strong>and</strong> the intervention type should be noted(such as “Enhancement <strong>of</strong> Recovery Readiness” group).3. Weekly progress notes must document the individual’s progress relative to functioning <strong>and</strong> skills related to the person-centered goals identified in his/her IRP. Thisprogress note aligns the weekly activities reported on the daily log or in daily notes to the stated interventions on the individualized recovery plan, <strong>and</strong> documentsprogress toward goals. The progress note may be written by any practitioner who provided services over the course <strong>of</strong> that week.4. If a daily log format is utilized, the consumer <strong>and</strong> Program Supervisor are required to sign the log once per week. The Supervisor’s signature is an attestation thatthe daily activities documented did indeed occur over the course <strong>of</strong> that week. The consumer should also sign the log (if the consumer refuses, documentation <strong>of</strong>his/her refusal would be indicated in the weekly summary).5. While billed in increments, the Peer Support service is a program model. Daily time in/time out is tracked for while the person is present in the program, but due totime/in out not being required for each intervention, the time in/out may not correlate with the units billed as the time in/out will include breaks taken during the course<strong>of</strong> the program. However, the units noted on the log should be consistent with the units billed <strong>and</strong>, if noted, on the weekly progress note. If the units documented arenot consistent, the most conservative number <strong>of</strong> units will be utilized <strong>and</strong> may result in a billing discrepancy.6. A provider shall only record units in which the consumer was actively engaged in services. Meals <strong>and</strong> breaks must not be included in the reporting <strong>of</strong> units <strong>of</strong> servicedelivered. Should a consumer leave the program or receive other services during the range <strong>of</strong> documented time in/time out for Peer Support hours, the absenceshould be documented on the log.Psychosocial RehabilitationTransactionCodePsychosocialRehabilitationCode Detail Code Mod Mod Mod Mod Rate Code Detail Code Mod Mod Mod Mod Rate1 2 3 41 2 3 4Practitioner Level 4, In-Clinic H2017 U4 U6 $4.43 Practitioner Level 4, Out-<strong>of</strong>-Clinic H2017 U4 U7 $5.41Practitioner Level 5, In-Clinic H2017 U5 U6 $3.30 Practitioner Level 5, Out-<strong>of</strong>-Clinic H2017 U5 U7 $4.03FY2013 Provider Manual for Community <strong>Behavioral</strong> <strong>Health</strong> Providers Page 116
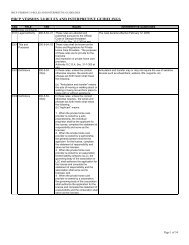
Psychosocial RehabilitationUnit Value Unit=15 minutes Maximum Daily Units 5 unitsInitial Auth 450 units Re-Authorization 450 unitsAuth Period 180 days Utilization Criteria LOCUS scores: 3-5A therapeutic, rehabilitative, skill building <strong>and</strong> recovery promoting service for individuals to gain the skills necessary to allow them to remain in or return to naturallyoccurring community settings <strong>and</strong> activities. Services include, but are not limited to:1) Individual or group skill building activities that focus on the development <strong>of</strong> skills to be used by individuals in their living, learning, social <strong>and</strong> working environments,2) Social, problem solving <strong>and</strong> coping skill development;3) Illness <strong>and</strong> medication self-management;4) Prevocational skills (for example: preparing for the workday; appropriate work attire <strong>and</strong> personal presentation including hygiene <strong>and</strong> use <strong>of</strong> personal effects suchas makeup, jewelry, perfume/cologne etc as appropriate to the work environment; time management; prioritizing tasks; taking direction from supervisors;appropriate use <strong>of</strong> break times <strong>and</strong> sick/personal leave; importance <strong>of</strong> learning <strong>and</strong> following the policies/rules <strong>and</strong> procedures <strong>of</strong> the workplace; workplace safety;problem solving/conflict resolution in the workplace; communication <strong>and</strong> relationships with coworkers <strong>and</strong> supervisors; resume <strong>and</strong> job application development;on-task behavior <strong>and</strong> task completion skills such as avoiding distraction from work tasks, following a task through to completion, asking for help when needed,Servicemaking sure deadlines are clarified <strong>and</strong> adhered to, etc; learning common work tasks or daily living tasks likely to be utilized in the workplace such as telephoneDefinitionskills, food preparation, organizing/filing, scheduling/participating in/leading meetings, computer skills etc) <strong>and</strong>5) Recreational activities/leisure skills that improve self-esteem <strong>and</strong> recovery.The programmatic goals <strong>of</strong> the service must be clearly articulated by the provider, utilizing a best/evidence based model for service delivery <strong>and</strong> support. Thesebest/evidence based models may include: the Boston University Psychosocial Rehabilitation approach, the Lieberman Model, the International Center for ClubhouseDevelopment approach, or blended models/approaches in accordance with current psychosocial rehabilitation research. Practitioners providing this service are expectedto maintain knowledge <strong>and</strong> skills regarding current research trends in best/evidence based models <strong>and</strong> practices for psychosocial rehabilitation.AdmissionCriteriaContinuingStay CriteriaDischargeCriteriaThis service is <strong>of</strong>fered in a group setting, though individual activities are allowable within the service when more circumstantially appropriate. Group activities <strong>and</strong>interventions should be made directly relevant to the needs, desires <strong>and</strong> IRP goals <strong>of</strong> the individual participants (i.e. an additional activity/group should be made availableas an alternative to a particular group for those individuals who do not need or wish to be in that group, as clinically appropriate).1. Individual must have primary behavioral health issues (including those with a co-occurring substance abuse disorder or MR/DD) <strong>and</strong> present a low or no risk <strong>of</strong> dangerto themselves or others; <strong>and</strong> one or more <strong>of</strong> the following:2. Individual lacks many functional <strong>and</strong> essential life skills such as daily living, social skills, vocational/academic skills <strong>and</strong>/or community/family integration; or3. Individual needs frequent assistance to obtain <strong>and</strong> use community resources.1. Primary behavioral health issues that continue to present a low or no imminent risk <strong>of</strong> danger to themselves or others (or is at risk <strong>of</strong> moderate to severe symptoms);<strong>and</strong> one or more <strong>of</strong> the following:2. Individual improvement in skills in some but not all areas; or3. If services are discontinued there would be an increase in symptoms <strong>and</strong> decrease in functioning1. An adequate continuing care plan has been established; <strong>and</strong> one or more <strong>of</strong> the following:2. Individual has acquired a significant number <strong>of</strong> needed skills; or3. Individual has sufficient knowledge <strong>and</strong> use <strong>of</strong> community supports; or4. Individual demonstrates ability to act on goals <strong>and</strong> is self sufficient or able to use peer supports for attainment <strong>of</strong> self sufficiency; orFY2013 Provider Manual for Community <strong>Behavioral</strong> <strong>Health</strong> Providers Page 117
- Page 1 and 2:
Georgia Department of Behavioral He
- Page 3 and 4:
UPDATED FOR JULY 1, 2013SUMMARY OF
- Page 5 and 6:
C&A Core ServicesBehavioral Health
- Page 7 and 8:
Community Supportsupports;9) Assist
- Page 9 and 10:
Community SupportServiceAccessibili
- Page 11 and 12:
Community Transition Planningv. App
- Page 13 and 14:
Diagnostic AssessmentTransactionCod
- Page 15 and 16:
Family Outpatient Services: Family
- Page 17 and 18:
Family Outpatient Services: Family
- Page 19 and 20:
Family Outpatient Services: Family
- Page 21 and 22:
Group Outpatient Services: Group Co
- Page 23 and 24:
Group Outpatient Services: Group Tr
- Page 25 and 26:
Individual CounselingServiceDefinit
- Page 27 and 28:
Medication AdministrationAdmissionC
- Page 29 and 30:
Nursing Assessment and Health Servi
- Page 31 and 32:
Continuing StayCriteriaDischargeCri
- Page 33 and 34:
Psychiatric TreatmentAdditionalMedi
- Page 35 and 36:
Service Plan DevelopmentPractitione
- Page 37 and 38:
CHILD & ADOLESCENT SPECIALTY SERVIC
- Page 39 and 40:
Behavioral AssistanceAssistance.Ser
- Page 41 and 42:
Crisis Stabilization Unit (CSU) Ser
- Page 43 and 44:
Crisis Stabilization Unit (CSU) Ser
- Page 45 and 46:
Intensive Family Intervention5. Bec
- Page 47 and 48:
Intensive Family Interventionconfid
- Page 49 and 50:
Intensive Family Intervention10. Th
- Page 51 and 52:
Structured Activity SupportsService
- Page 53 and 54:
Structured Residential SupportsClin
- Page 55 and 56:
Substance Abuse Intensive Outpatien
- Page 57 and 58:
Substance Abuse Intensive Outpatien
- Page 59 and 60:
Substance Abuse Intensive Outpatien
- Page 61 and 62:
RequiredComponents1. Any diagnosis
- Page 63 and 64:
Community Support3. Contact must be
- Page 65 and 66: Community Transition Planning3. Jai
- Page 67 and 68: ContinuingStay CriteriaDischargeCri
- Page 69 and 70: Family Outpatient Services: Family
- Page 71 and 72: Family Outpatient Services: Family
- Page 73 and 74: Family Outpatient Services: Family
- Page 75 and 76: Group Outpatient Services: Group Co
- Page 77 and 78: Group Outpatient Services: Group Tr
- Page 79 and 80: Individual CounselingServiceDefinit
- Page 81 and 82: StaffingRequirementsServiceAccessib
- Page 83 and 84: Medication Administrationliving.Req
- Page 85 and 86: Nursing Assessment and Health Servi
- Page 87 and 88: Psychiatric Treatmentbehaviormodify
- Page 89 and 90: Psychological Testing: Psychologica
- Page 91 and 92: Service Plan DevelopmentRecovery pl
- Page 93 and 94: Ambulatory Substance Abuse Detoxifi
- Page 95 and 96: Assertive Community Treatmente. Ass
- Page 97 and 98: Assertive Community Treatment• Di
- Page 99 and 100: Assertive Community Treatment• di
- Page 101 and 102: Assertive Community Treatment11. Fo
- Page 103 and 104: Assertive Community Treatmentin whi
- Page 105 and 106: Consumer/Family AssistanceTransacti
- Page 107 and 108: Consumer/Family Assistancecriticaln
- Page 109 and 110: Crisis Stabilization Unit Servicesb
- Page 111 and 112: ClinicalExclusionsDocumentationRequ
- Page 113 and 114: Peer Support Services4. Individual
- Page 115: Peer Support ServicesClinicalOperat
- Page 119 and 120: Psychosocial Rehabilitationmust dem
- Page 121 and 122: Psychosocial RehabilitationBilling
- Page 123 and 124: Residential: Independent Residentia
- Page 125 and 126: Residential: Intensive Residential
- Page 127 and 128: Residential: Semi-Independent Resid
- Page 129 and 130: Residential Substance Detoxificatio
- Page 131 and 132: ServiceDefinitionAdmissionCriteriaC
- Page 133 and 134: AdmissionCriteria,continuedContinui
- Page 135 and 136: 1. It is expected that the transiti
- Page 137 and 138: DocumentationRequirements1. Every a
- Page 139 and 140: FY2013 Provider Manual for Communit
- Page 141 and 142: TABLE B: Physicians, Physician’s
- Page 143 and 144: COMMUNITY SERVICE STANDARDS FOR ALL
- Page 145 and 146: 3. The provider details the desired
- Page 147 and 148: 7. The provider’s practice of cul
- Page 149 and 150: c. Is not permitted in developmenta
- Page 151 and 152: 2. Policies, procedures, and guidel
- Page 153 and 154: 3. Safe transport of persons served
- Page 155 and 156: iv. There are safeguards utilized f
- Page 157 and 158: i. The date and time the medication
- Page 159 and 160: Training Requirements for all Staff
- Page 161 and 162: Qualified MedicationAide (QMA)Psych
- Page 163 and 164: Addiction CounselorTrainees (ACT)Hi
- Page 165 and 166: CADC, CCADC, CAC II or MAC and is r
- Page 167 and 168:
practitioner), s/he could bill as a
- Page 169 and 170:
COMMUNITY SERVICE STANDARDS FOR ALL
- Page 171 and 172:
4. ORDER/RECOMMENDATION FOR COURSE
- Page 173 and 174:
ii. Services, supports, and treatme
- Page 175 and 176:
xv.xvi.xvii.Recorded changes - Any