Psychiatric TreatmentServiceExclusionsClinicalExclusionsRequiredComponentsClinicalOperationsServiceAccessibilityAdditionalMedicaidRequirementsReporting <strong>and</strong>BillingRequirementsNot <strong>of</strong>fered in conjunction with ACTServices defined as a part <strong>of</strong> ACTTelemedicine may be utilized for an initial Psychiatric Diagnostic Examination as well as for ongoing Psychiatric Diagnostic Examination via the use <strong>of</strong> appropriateprocedure codes with the GT modifier.1. In accordance with recovery philosophy, it is expected that individuals will be treated as full partners in the treatment regimen/services planned <strong>and</strong> received.As such, it is expected that practitioners will fully discuss treatment options with individuals <strong>and</strong> allow for individual choice when possible. Discussion <strong>of</strong> treatmentoptions should include a full disclosure <strong>of</strong> the pros <strong>and</strong> cons <strong>of</strong> each option (e.g. full disclosure <strong>of</strong> medication/treatment regimen potential side effects, potentialadverse reactions--including potential adverse reaction from not taking medication as prescribed, <strong>and</strong> expected benefits). If such full discussion/disclosure is notpossible or advisable according to the clinical judgment <strong>of</strong> the practitioner, this should be documented in the individual’s chart (including the specific information thatwas not discussed <strong>and</strong> a compelling rationale for lack <strong>of</strong> discussion/disclosure).2. Assistive tools, technologies, worksheets, etc. can be used by the served individual to facilitate communication about treatment, symptoms, improvements, etc.with the treating practitioner.Telemedicine is the use <strong>of</strong> medical information exchanged from one site to another via electronic communications to improve a patient's health. Electroniccommunication means the use <strong>of</strong> interactive telecommunications equipment that includes, at a minimum, audio <strong>and</strong> video equipment permitting two-way, real timeinteractive communication between the patient, <strong>and</strong> the physician or practitioner at the distant site.1. The daily maximum within a CSU for Pharmacologic Management is 1 unit/day.2. Even if a physician also has his/her own Medicaid number, the physician providing behavioral health treatment <strong>and</strong> care through this code should bill via theapproved provider agency’s Medicaid number through the Medicaid Category <strong>of</strong> Service (COS) 440.1. Within this service group, a second unit with a U1 modifier may be used in the event that a Telemedicine Psychiatric Treatment unit is provided <strong>and</strong> it indicates aneed for a face-to-face assessment (e.g. 90862GTU1 is billed <strong>and</strong> it is clinically indicated that a face-to-face by an on-site physician needs to immediately followbased upon clinical indicators during the first intervention, then 90862U1, can also be billed in the same day).2. Within this service group, there is an allowance for when a U2 practitioner conducts an intervention <strong>and</strong>, because <strong>of</strong> clinical indicators presenting during thisintervention, a U1 practitioner needs to provide another unit due to the concern <strong>of</strong> the U2 supervisee (e.g. Physician’s Assistant provides <strong>and</strong> bills 90805U2U6 <strong>and</strong>because <strong>of</strong> concerns, requests U1 intervention following his/her billing <strong>of</strong> U2 intervention). The use <strong>of</strong> this practice should be rare <strong>and</strong> will be subject to additionalutilization review scrutiny.FY2013 Provider Manual for Community <strong>Behavioral</strong> <strong>Health</strong> Providers Page 88
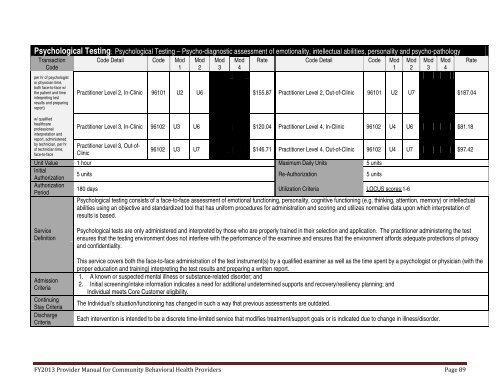
Psychological Testing: Psychological Testing – Psycho-diagnostic assessment <strong>of</strong> emotionality, intellectual abilities, personality <strong>and</strong> psycho-pathologyTransactionCodeper hr <strong>of</strong> psychologistor physician time,both face-to-face w/the patient <strong>and</strong> timeinterpreting testresults <strong>and</strong> preparingreport)w/ qualifiedhealthcarepr<strong>of</strong>essionalinterpretation <strong>and</strong>report, administeredby technician, per hr<strong>of</strong> technician time,face-to-faceCode Detail Code Mod1Mod2Mod3Mod4Rate Code Detail Code Mod1Practitioner Level 2, In-Clinic 96101 U2 U6 $155.87 Practitioner Level 2, Out-<strong>of</strong>-Clinic 96101 U2 U7 $187.04Practitioner Level 3, In-Clinic 96102 U3 U6 $120.04 Practitioner Level 4, In-Clinic 96102 U4 U6 $81.18Practitioner Level 3, Out-<strong>of</strong>-Clinic96102 U3 U7 $146.71 Practitioner Level 4, Out-<strong>of</strong>-Clinic 96102 U4 U7 $97.42Unit Value 1 hour Maximum Daily Units 5 unitsInitialAuthorization5 units Re-Authorization 5 unitsAuthorizationPeriod180 days Utilization Criteria LOCUS scores:1-6Psychological testing consists <strong>of</strong> a face-to-face assessment <strong>of</strong> emotional functioning, personality, cognitive functioning (e.g. thinking, attention, memory) or intellectualabilities using an objective <strong>and</strong> st<strong>and</strong>ardized tool that has uniform procedures for administration <strong>and</strong> scoring <strong>and</strong> utilizes normative data upon which interpretation <strong>of</strong>results is based.Mod2Mod3Mod4RateServiceDefinitionAdmissionCriteriaContinuingStay CriteriaDischargeCriteriaPsychological tests are only administered <strong>and</strong> interpreted by those who are properly trained in their selection <strong>and</strong> application. The practitioner administering the testensures that the testing environment does not interfere with the performance <strong>of</strong> the examinee <strong>and</strong> ensures that the environment affords adequate protections <strong>of</strong> privacy<strong>and</strong> confidentiality.This service covers both the face-to-face administration <strong>of</strong> the test instrument(s) by a qualified examiner as well as the time spent by a psychologist or physician (with theproper education <strong>and</strong> training) interpreting the test results <strong>and</strong> preparing a written report.1. A known or suspected mental illness or substance-related disorder; <strong>and</strong>2. Initial screening/intake information indicates a need for additional undetermined supports <strong>and</strong> recovery/resiliency planning; <strong>and</strong>Individual meets Core Customer eligibility.The Individual’s situation/functioning has changed in such a way that previous assessments are outdated.Each intervention is intended to be a discrete time-limited service that modifies treatment/support goals or is indicated due to change in illness/disorder.FY2013 Provider Manual for Community <strong>Behavioral</strong> <strong>Health</strong> Providers Page 89
- Page 1 and 2:
Georgia Department of Behavioral He
- Page 3 and 4:
UPDATED FOR JULY 1, 2013SUMMARY OF
- Page 5 and 6:
C&A Core ServicesBehavioral Health
- Page 7 and 8:
Community Supportsupports;9) Assist
- Page 9 and 10:
Community SupportServiceAccessibili
- Page 11 and 12:
Community Transition Planningv. App
- Page 13 and 14:
Diagnostic AssessmentTransactionCod
- Page 15 and 16:
Family Outpatient Services: Family
- Page 17 and 18:
Family Outpatient Services: Family
- Page 19 and 20:
Family Outpatient Services: Family
- Page 21 and 22:
Group Outpatient Services: Group Co
- Page 23 and 24:
Group Outpatient Services: Group Tr
- Page 25 and 26:
Individual CounselingServiceDefinit
- Page 27 and 28:
Medication AdministrationAdmissionC
- Page 29 and 30:
Nursing Assessment and Health Servi
- Page 31 and 32:
Continuing StayCriteriaDischargeCri
- Page 33 and 34:
Psychiatric TreatmentAdditionalMedi
- Page 35 and 36:
Service Plan DevelopmentPractitione
- Page 37 and 38: CHILD & ADOLESCENT SPECIALTY SERVIC
- Page 39 and 40: Behavioral AssistanceAssistance.Ser
- Page 41 and 42: Crisis Stabilization Unit (CSU) Ser
- Page 43 and 44: Crisis Stabilization Unit (CSU) Ser
- Page 45 and 46: Intensive Family Intervention5. Bec
- Page 47 and 48: Intensive Family Interventionconfid
- Page 49 and 50: Intensive Family Intervention10. Th
- Page 51 and 52: Structured Activity SupportsService
- Page 53 and 54: Structured Residential SupportsClin
- Page 55 and 56: Substance Abuse Intensive Outpatien
- Page 57 and 58: Substance Abuse Intensive Outpatien
- Page 59 and 60: Substance Abuse Intensive Outpatien
- Page 61 and 62: RequiredComponents1. Any diagnosis
- Page 63 and 64: Community Support3. Contact must be
- Page 65 and 66: Community Transition Planning3. Jai
- Page 67 and 68: ContinuingStay CriteriaDischargeCri
- Page 69 and 70: Family Outpatient Services: Family
- Page 71 and 72: Family Outpatient Services: Family
- Page 73 and 74: Family Outpatient Services: Family
- Page 75 and 76: Group Outpatient Services: Group Co
- Page 77 and 78: Group Outpatient Services: Group Tr
- Page 79 and 80: Individual CounselingServiceDefinit
- Page 81 and 82: StaffingRequirementsServiceAccessib
- Page 83 and 84: Medication Administrationliving.Req
- Page 85 and 86: Nursing Assessment and Health Servi
- Page 87: Psychiatric Treatmentbehaviormodify
- Page 91 and 92: Service Plan DevelopmentRecovery pl
- Page 93 and 94: Ambulatory Substance Abuse Detoxifi
- Page 95 and 96: Assertive Community Treatmente. Ass
- Page 97 and 98: Assertive Community Treatment• Di
- Page 99 and 100: Assertive Community Treatment• di
- Page 101 and 102: Assertive Community Treatment11. Fo
- Page 103 and 104: Assertive Community Treatmentin whi
- Page 105 and 106: Consumer/Family AssistanceTransacti
- Page 107 and 108: Consumer/Family Assistancecriticaln
- Page 109 and 110: Crisis Stabilization Unit Servicesb
- Page 111 and 112: ClinicalExclusionsDocumentationRequ
- Page 113 and 114: Peer Support Services4. Individual
- Page 115 and 116: Peer Support ServicesClinicalOperat
- Page 117 and 118: Psychosocial RehabilitationUnit Val
- Page 119 and 120: Psychosocial Rehabilitationmust dem
- Page 121 and 122: Psychosocial RehabilitationBilling
- Page 123 and 124: Residential: Independent Residentia
- Page 125 and 126: Residential: Intensive Residential
- Page 127 and 128: Residential: Semi-Independent Resid
- Page 129 and 130: Residential Substance Detoxificatio
- Page 131 and 132: ServiceDefinitionAdmissionCriteriaC
- Page 133 and 134: AdmissionCriteria,continuedContinui
- Page 135 and 136: 1. It is expected that the transiti
- Page 137 and 138: DocumentationRequirements1. Every a
- Page 139 and 140:
FY2013 Provider Manual for Communit
- Page 141 and 142:
TABLE B: Physicians, Physician’s
- Page 143 and 144:
COMMUNITY SERVICE STANDARDS FOR ALL
- Page 145 and 146:
3. The provider details the desired
- Page 147 and 148:
7. The provider’s practice of cul
- Page 149 and 150:
c. Is not permitted in developmenta
- Page 151 and 152:
2. Policies, procedures, and guidel
- Page 153 and 154:
3. Safe transport of persons served
- Page 155 and 156:
iv. There are safeguards utilized f
- Page 157 and 158:
i. The date and time the medication
- Page 159 and 160:
Training Requirements for all Staff
- Page 161 and 162:
Qualified MedicationAide (QMA)Psych
- Page 163 and 164:
Addiction CounselorTrainees (ACT)Hi
- Page 165 and 166:
CADC, CCADC, CAC II or MAC and is r
- Page 167 and 168:
practitioner), s/he could bill as a
- Page 169 and 170:
COMMUNITY SERVICE STANDARDS FOR ALL
- Page 171 and 172:
4. ORDER/RECOMMENDATION FOR COURSE
- Page 173 and 174:
ii. Services, supports, and treatme
- Page 175 and 176:
xv.xvi.xvii.Recorded changes - Any