

url?sa=t&source=web&cd=2&ved=0CC0QFjAB&url=http://filletofish.net/usc/Pocket_Medicine_4th_Edition
url?sa=t&source=web&cd=2&ved=0CC0QFjAB&url=http://filletofish.net/usc/Pocket_Medicine_4th_Edition
url?sa=t&source=web&cd=2&ved=0CC0QFjAB&url=http://filletofish.net/usc/Pocket_Medicine_4th_Edition

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
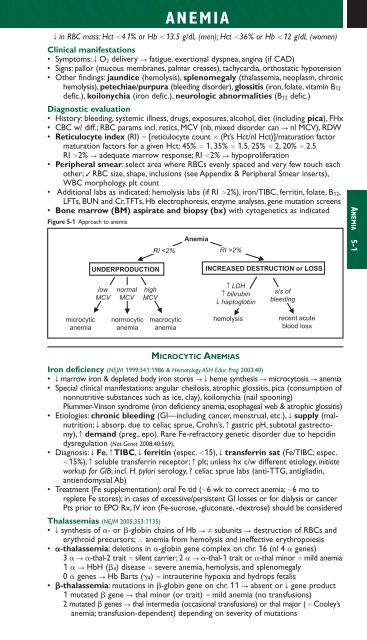
ANEMIAT in RBC mass: Hct 41% or Hb 13.5 g/dL (men); Hct 36% or Hb 12 g/dL (women)Clinical manifestations• Symptoms: T O 2 delivery S fatigue, exertional dyspnea, angina (if CAD)• Signs: pallor (mucous membranes, palmar creases), tachycardia, orthostatic hypotension• Other findings: jaundice (hemolysis), splenomegaly (thalassemia, neoplasm, chronichemolysis), petechiae/purpura (bleeding disorder), glossitis (iron, folate, vitamin B 12defic.), koilonychia (iron defic.), neurologic abnormalities (B 12 defic.)Diagnostic evaluation• History: bleeding, systemic illness, drugs, exposures, alcohol, diet (including pica), FHx• CBC w/ diff.; RBC params incl. retics, MCV (nb, mixed disorder can S nl MCV), RDW• Reticulocyte index (RI) [reticulocyte count (Pt’s Hct/nl Hct)]/maturation factormaturation factors for a given Hct: 45% 1, 35% 1.5, 25% 2, 20% 2.5RI 2% S adequate marrow response; RI 2% S hypoproliferation• Peripheral smear: select area where RBCs evenly spaced and very few touch eachother; ✓ RBC size, shape, inclusions (see Appendix & Peripheral Smear inserts),WBC morphology, plt count• Additional labs as indicated: hemolysis labs (if RI 2%), iron/TIBC, ferritin, folate, B 12,LFTs, BUN and Cr,TFTs, Hb electrophoresis, enzyme analyses, gene mutation screens• Bone marrow (BM) aspirate and biopsy (bx) with cytoge<strong>net</strong>ics as indicatedFigure 5-1 Approach to anemiaRI 2%ANEMIA 5-1UNDERPRODUCTIONINCREASED DESTRUCTION or LOSSlowMCVnormalMCVhighMCV↑ LDH↑ bilirubin↓ haptoglobins/s ofbleedingmicrocyticanemianormocyticanemiamacrocyticanemiahemolysisrecent acuteblood lossMICROCYTIC ANEMIASIron deficiency (NEJM 1999;341:1986 & Hematology ASH Educ Prog 2003;40)• T marrow iron & depleted body iron stores STheme synthesis S microcytosis S anemia• Special clinical manifestations: angular cheilosis, atrophic glossitis, pica (consumption ofnonnutritive substances such as ice, clay), koilonychia (nail spooning)Plummer-Vinson syndrome (iron deficiency anemia, esophageal web & atrophic glossitis)• Etiologies: chronic bleeding (GI—including cancer, menstrual, etc.), T supply (malnutrition;T absorp. due to celiac sprue, Crohn’s, c gastric pH, subtotal gastrectomy),c demand (preg., epo). Rare Fe-refractory ge<strong>net</strong>ic disorder due to hepcidindysregulation (Nat Ge<strong>net</strong> 2008;40:569).• Diagnosis: T Fe, c TIBC, T ferritin (espec. 15), T transferrin sat (Fe/TIBC; espec.15%), c soluble transferrin receptor; c plt; unless hx c/w different etiology, initiateworkup for GIB; incl. H. pylori serology, ? celiac sprue labs (anti-TTG, antigliadin,antiendomysial Ab)• Treatment (Fe supplementation): oral Fe tid (6 wk to correct anemia; 6 mo toreplete Fe stores); in cases of excessive/persistent GI losses or for dialysis or cancerPts prior to EPO Rx, IV iron (Fe-sucrose, -gluconate, -dextrose) should be consideredThalassemias (NEJM 2005;353:1135)• T synthesis of - or -globin chains of Hb S Z subunits S destruction of RBCs anderythroid precursors; ∴ anemia from hemolysis and ineffective erythropoiesis• -thalassemia: deletions in -globin gene complex on chr. 16 (nl 4 genes)3 S -thal-2 trait silent carrier; 2 S -thal-1 trait or -thal minor mild anemia1 S HbH ( 4) disease severe anemia, hemolysis, and splenomegaly0 genes S Hb Barts ( 4) intrauterine hypoxia and hydrops fetalis• -thalassemia: mutations in -globin gene on chr. 11 S absent or T gene product1 mutated gene S thal minor (or trait) mild anemia (no transfusions)2 mutated genes S thal intermedia (occasional transfusions) or thal major ( Cooley’sanemia; transfusion-dependent) depending on severity of mutations