

url?sa=t&source=web&cd=2&ved=0CC0QFjAB&url=http://filletofish.net/usc/Pocket_Medicine_4th_Edition
url?sa=t&source=web&cd=2&ved=0CC0QFjAB&url=http://filletofish.net/usc/Pocket_Medicine_4th_Edition
url?sa=t&source=web&cd=2&ved=0CC0QFjAB&url=http://filletofish.net/usc/Pocket_Medicine_4th_Edition

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
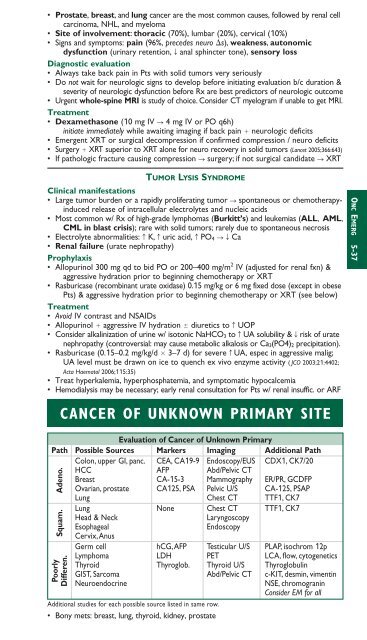
• Prostate, breast, and lung cancer are the most common causes, followed by renal cellcarcinoma, NHL, and myeloma• Site of involvement: thoracic (70%), lumbar (20%), cervical (10%)• Signs and symptoms: pain (96%, precedes neuro s), weakness, autonomicdysfunction (urinary retention, T anal sphincter tone), sensory lossDiagnostic evaluation• Always take back pain in Pts with solid tumors very seriously• Do not wait for neurologic signs to develop before initiating evaluation b/c duration &severity of neurologic dysfunction before Rx are best predictors of neurologic outcome• Urgent whole-spine MRI is study of choice. Consider CT myelogram if unable to get MRI.Treatment• Dexamethasone (10 mg IV S 4 mg IV or PO q6h)initiate immediately while awaiting imaging if back pain neurologic deficits• Emergent XRT or surgical decompression if confirmed compression / neuro deficits• Surgery XRT superior to XRT alone for neuro recovery in solid tumors (Lancet 2005;366:643)• If pathologic fracture causing compression S surgery; if not surgical candidate S XRTTUMOR LYSIS SYNDROMEClinical manifestations• Large tumor burden or a rapidly proliferating tumor S spontaneous or chemotherapyinducedrelease of intracellular electrolytes and nucleic acids• Most common w/ Rx of high-grade lymphomas (Burkitt’s) and leukemias (ALL, AML,CML in blast crisis); rare with solid tumors; rarely due to spontaneous necrosis• Electrolyte abnormalities: c K, c uric acid, c PO 4 STCa• Renal failure (urate nephropathy)Prophylaxis• Allopurinol 300 mg qd to bid PO or 200–400 mg/m 2 IV (adjusted for renal fxn) &aggressive hydration prior to beginning chemotherapy or XRT• Rasburicase (recombinant urate oxidase) 0.15 mg/kg or 6 mg fixed dose (except in obesePts) & aggressive hydration prior to beginning chemotherapy or XRT (see below)Treatment• Avoid IV contrast and NSAIDs• Allopurinol aggressive IV hydration diuretics to c UOP• Consider alkalinization of urine w/ isotonic NaHCO 3 to c UA solubility & T risk of uratenephropathy (controversial: may cause metabolic alkalosis or Ca 3(PO4) 2 precipitation).• Rasburicase (0.15–0.2 mg/kg/d 3–7 d) for severe c UA, espec in aggressive malig;UA level must be drawn on ice to quench ex vivo enzyme activity ( JCO 2003;21:4402;Acta Haematol 2006;115:35)• Treat hyperkalemia, hyperphosphatemia, and symptomatic hypocalcemia• Hemodialysis may be necessary; early renal consultation for Pts w/ renal insuffic. or ARFCANCER OF UNKNOWN PRIMARY SITEEvaluation of Cancer of Unknown PrimaryPath Possible Sources Markers Imaging Additional PathColon, upper GI, panc. CEA, CA19-9 Endoscopy/EUS CDX1, CK7/20HCC AFP Abd/Pelvic CTBreast CA-15-3 Mammography ER/PR, GCDFPOvarian, prostate CA125, PSA Pelvic U/S CA-125, PSAPLung Chest CT TTF1, CK7Lung None Chest CT TTF1, CK7Head & NeckLaryngoscopySquam. Adeno.PoorlyDifferen.EsophagealEndoscopyCervix,AnusGerm cell hCG,AFP Testicular U/S PLAP, isochrom 12pLymphoma LDH PET LCA, flow, cytoge<strong>net</strong>icsThyroid Thyroglob. Thyroid U/S ThyroglobulinGIST, Sarcoma Abd/Pelvic CT c-KIT, desmin, vimentinNeuroendocrineAdditional studies for each possible source listed in same row.• Bony mets: breast, lung, thyroid, kidney, prostateNSE, chromograninConsider EM for allONC EMERG 5-37