

url?sa=t&source=web&cd=2&ved=0CC0QFjAB&url=http://filletofish.net/usc/Pocket_Medicine_4th_Edition
url?sa=t&source=web&cd=2&ved=0CC0QFjAB&url=http://filletofish.net/usc/Pocket_Medicine_4th_Edition
url?sa=t&source=web&cd=2&ved=0CC0QFjAB&url=http://filletofish.net/usc/Pocket_Medicine_4th_Edition

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
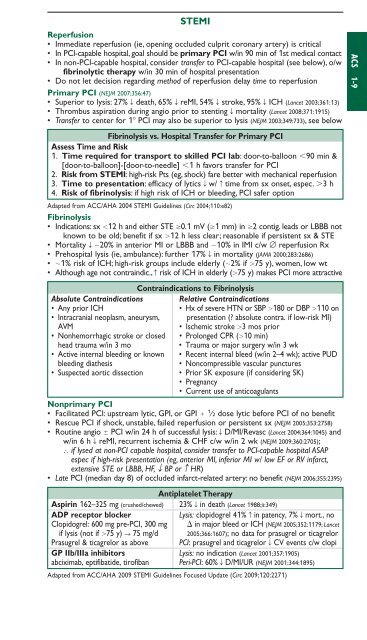
STEMIReperfusion• Immediate reperfusion (ie, opening occluded culprit coronary artery) is critical• In PCI-capable hospital, goal should be primary PCI w/in 90 min of 1st medical contact• In non-PCI-capable hospital, consider transfer to PCI-capable hospital (see below), o/wfibrinolytic therapy w/in 30 min of hospital presentation• Do not let decision regarding method of reperfusion delay time to reperfusionPrimary PCI (NEJM 2007;356:47)• Superior to lysis: 27% T death, 65% T reMI, 54% T stroke, 95% T ICH (Lancet 2003;361:13)• Thrombus aspiration during angio prior to stenting T mortality (Lancet 2008;371:1915)• Transfer to center for 1 PCI may also be superior to lysis (NEJM 2003;349:733), see belowFibrinolysis vs. Hospital Transfer for Primary PCIAssess Time and Risk1. Time required for transport to skilled PCI lab: door-to-balloon 90 min &[door-to-balloon]-[door-to-needle] 1 h favors transfer for PCI2. Risk from STEMI: high-risk Pts (eg, shock) fare better with mechanical reperfusion3. Time to presentation: efficacy of lytics T w/ c time from sx onset, espec. 3 h4. Risk of fibrinolysis: if high risk of ICH or bleeding, PCI safer optionAdapted from ACC/AHA 2004 STEMI Guidelines (Circ 2004;110:e82)Fibrinolysis• Indications: sx 12 h and either STE 0.1 mV (1 mm) in 2 contig. leads or LBBB notknown to be old; benefit if sx 12 h less clear; reasonable if persistent sx & STE• Mortality T 20% in anterior MI or LBBB and 10% in IMI c/w ∅ reperfusion Rx• Prehospital lysis (ie, ambulance): further 17% T in mortality (JAMA 2000;283:2686)• 1% risk of ICH; high-risk groups include elderly (2% if 75 y), women, low wt• Although age not contraindic., c risk of ICH in elderly (75 y) makes PCI more attractiveContraindications to FibrinolysisAbsolute Contraindications Relative Contraindications• Any prior ICH• Hx of severe HTN or SBP 180 or DBP 110 on• Intracranial neoplasm, aneurysm, presentation (? absolute contra. if low-risk MI)AVM• Ischemic stroke 3 mos prior• Nonhemorrhagic stroke or closed • Prolonged CPR (10 min)head trauma w/in 3 mo• Trauma or major surgery w/in 3 wk• Active internal bleeding or known • Recent internal bleed (w/in 2–4 wk); active PUDbleeding diathesis• Noncompressible vascular punctures• Suspected aortic dissection • Prior SK exposure (if considering SK)• Pregnancy• Current use of anticoagulantsNonprimary PCI• Facilitated PCI: upstream lytic, GPI, or GPI 1 ⁄2 dose lytic before PCI of no benefit• Rescue PCI if shock, unstable, failed reperfusion or persistent sx (NEJM 2005;353:2758)• Routine angio PCI w/in 24 h of successful lysis: T D/MI/Revasc (Lancet 2004;364:1045) andw/in 6 h T reMI, recurrent ischemia & CHF c/w w/in 2 wk (NEJM 2009;360:2705);∴ if lysed at non-PCI capable hospital, consider transfer to PCI-capable hospital ASAPespec if high-risk presentation (eg, anterior MI, inferior MI w/ low EF or RV infarct,extensive STE or LBBB, HF, T BP or c HR)• Late PCI (median day 8) of occluded infarct-related artery: no benefit (NEJM 2006;355:2395)Antiplatelet TherapyAspirin 162–325 mg (crushed/chewed) 23% T in death (Lancet 1988;ii:349)ADP receptor blockerLysis: clopidogrel 41% c in patency, 7% T mort., noClopidogrel: 600 mg pre-PCI, 300 mg in major bleed or ICH (NEJM 2005;352:1179; Lancetif lysis (not if 75 y) S 75 mg/d 2005;366:1607); no data for prasugrel or ticagrelorPrasugrel & ticagrelor as above PCI: prasugrel and ticagrelor T CV events c/w clopiGP IIb/IIIa inhibitors Lysis: no indication (Lancet 2001;357:1905)abciximab, eptifibatide, tirofiban Peri-PCI: 60% T D/MI/UR (NEJM 2001;344:1895)Adapted from ACC/AHA 2009 STEMI Guidelines Focused Update (Circ 2009;120:2271)ACS 1-9