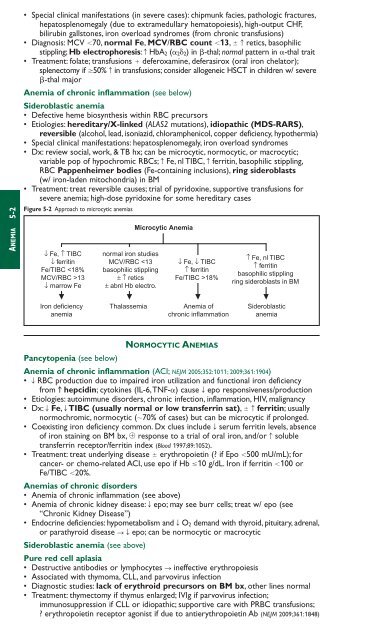
ANEMIA 5-2• Special clinical manifestations (in severe cases): chipmunk facies, pathologic fractures,hepatosplenomegaly (due to extramedullary hematopoiesis), high-output CHF,bilirubin gallstones, iron overload syndromes (from chronic transfusions)• Diagnosis: MCV 70, normal Fe, MCV/RBC count 13, c retics, basophilicstippling; Hb electrophoresis: c HbA 2 ( 2 2) in -thal; normal pattern in -thal trait• Treatment: folate; transfusions deferoxamine, deferasirox (oral iron chelator);splenectomy if 50% c in transfusions; consider allogeneic HSCT in children w/ severe-thal majorAnemia of chronic inflammation (see below)Sideroblastic anemia• Defective heme biosynthesis within RBC precursors• Etiologies: hereditary/X-linked (ALAS2 mutations), idiopathic (MDS-RARS),reversible (alcohol, lead, isoniazid, chloramphenicol, copper deficiency, hypothermia)• Special clinical manifestations: hepatosplenomegaly, iron overload syndromes• Dx: review social, work, & TB hx; can be microcytic, normocytic, or macrocytic;variable pop of hypochromic RBCs; c Fe, nl TIBC, c ferritin, basophilic stippling,RBC Pappenheimer bodies (Fe-containing inclusions), ring sideroblasts(w/ iron-laden mitochondria) in BM• Treatment: treat reversible causes; trial of pyridoxine, supportive transfusions forsevere anemia; high-dose pyridoxine for some hereditary casesFigure 5-2 Approach to microcytic anemias↓ Fe, ↑ TIBC↓ ferritinFe/TIBC 13↓ marrow Fenormal iron studiesMCV/RBC 18%↑ Fe, nl TIBC↑ ferritinbasophilic stipplingring sideroblasts in BMIron deficiencyanemiaThalassemiaAnemia ofchronic inflammationSideroblasticanemiaPancytopenia (see below)NORMOCYTIC ANEMIASAnemia of chronic inflammation (ACI; NEJM 2005;352:1011; 2009;361:1904)• T RBC production due to impaired iron utilization and functional iron deficiencyfrom c hepcidin; cytokines (IL-6,TNF-) cause T epo responsiveness/production• Etiologies: autoimmune disorders, chronic infection, inflammation, HIV, malignancy• Dx: T Fe, T TIBC (usually normal or low transferrin sat), c ferritin; usuallynormochromic, normocytic (70% of cases) but can be microcytic if prolonged.• Coexisting iron deficiency common. Dx clues include T serum ferritin levels, absenceof iron staining on BM bx, response to a trial of oral iron, and/or c solubletransferrin receptor/ferritin index (Blood 1997;89:1052).• Treatment: treat underlying disease erythropoietin (? if Epo 500 mU/mL); forcancer- or chemo-related ACI, use epo if Hb 10 g/dL. Iron if ferritin 100 orFe/TIBC 20%.Anemias of chronic disorders• Anemia of chronic inflammation (see above)• Anemia of chronic kidney disease: T epo; may see burr cells; treat w/ epo (see“Chronic Kidney Disease”)• Endocrine deficiencies: hypometabolism and T O 2 demand with thyroid, pituitary, adrenal,or parathyroid disease STepo; can be normocytic or macrocyticSideroblastic anemia (see above)Pure red cell aplasia• Destructive antibodies or lymphocytes S ineffective erythropoiesis• Associated with thymoma, CLL, and parvovirus infection• Diagnostic studies: lack of erythroid precursors on BM bx, other lines normal• Treatment: thymectomy if thymus enlarged; IVIg if parvovirus infection;immunosuppression if CLL or idiopathic; supportive care with PRBC transfusions;? erythropoietin receptor agonist if due to antierythropoietin Ab (NEJM 2009;361:1848)
MACROCYTIC ANEMIASincludes megaloblastic and nonmegaloblastic causesMegaloblastic anemia• Impaired DNA synthesis S cytoplasm matures faster than nucleus S ineffectiveerythropoiesis and macrocytosis; due to folate or B 12 deficiency• ✓ folate and vitamin B 12, c LDH & indirect bilirubin (due to ineffective erythropoiesis)• Smear: neutrophil hypersegmentation, macro-ovalocytes, anisocytosis, poikilocytosisFolate deficiency• Folate present in leafy green vegetables and fruit; total body stores sufficient for 2–3 mo• Etiologies: malnutrition (alcoholics, anorectics, elderly), T absorption (sprue),impaired metabolism (methotrexate, pyrimethamine, trimethoprim), c requirement(chronic hemolytic anemia, pregnancy, malignancy, dialysis)• Diagnosis: T folate; T RBC folate, c homocyst. but nl methylmalonic acid (unlike B 12 defic.)• Treatment: folate 1–5 mg PO qd for 1–4 mo or until complete hematologic recovery;critical to r/o B 12 deficiency first (see below)Vitamin B 12 deficiency• B 12 present only in foods of animal origin; total body stores sufficient for 2–3 y• Binds to intrinsic factor (IF) secreted by gastric parietal cells; absorbed in terminal ileum• Etiologies: malnutrition (alcoholics, vegans), pernicious anemia (PA, autoimmune diseaseagainst gastric parietal cells, a/w polyglandular endocrine insufficiency and crisk of gastric carcinoma), other causes of T absorption (gastrectomy, sprue, Crohn’sdisease), c competition (intestinal bacterial overgrowth, fish tapeworm)• Clinical manifestations: neurologic changes (subacute combined degeneration)affecting peripheral nerves, posterior and lateral columns of the spinal cord, and cortexS numbness, paresthesias, T vibratory and positional sense, ataxia, dementia• Dx: T B 12; c homocysteine and methylmalonic acid; anti-IF Ab; Schilling test; c gastrin in PA• Treatment: 1 mg B 12 IM qd 7 d S q wk 4–8 wk S q month for lifeneurologic abnormalities are reversible if treated w/in 6 mofolate can reverse hematologic abnormalities of B 12 deficiency but not neurologicchanges (and can lead to “steal” of B 12 stores S worsening of neuro complications)oral supplementation (2 mg qd) appears feasible as well (Blood 1998;92:1191) even w/o IFNonmegaloblastic macrocytic anemias• Liver disease: often macrocytic, may see target cells• Alcoholism: BM suppression & macrocytosis independent of folate/B 12 defic. or cirrhosis• Reticulocytosis• Other causes: hypothyroidism; MDS; meds that impair DNA synthesis (zidovudine,5-FU, hydroxyurea,Ara-C); hereditary orotic aciduria; Lesch-Nyhan synd.ANEMIA 5-3PANCYTOPENIAEtiologies• Hypocellular bone marrow (nl cellularity 100 – age): aplastic anemia, hypoplastic MDS• Cellular bone marrow: MDS, aleukemic leukemia, PNH, severe megaloblastic anemia• Marrow replacement (myelophthisis): myelofibrosis, metastatic solid tumors, granulomas• Systemic diseases: hypersplenism, sepsis, alcohol, toxinsClinical manifestations• Anemia S fatigue• Neutropenia S recurrent infections• Thrombocytopenia S mucosal bleeding & easy bruisabilityAplastic anemia stem cell failure (Lancet 2005;365:1647)• Epidemiology: 2–5 cases/10 6 /y; biphasic (major peak in adolescents, 2nd peak in elderly)• Diagnosis: pancytopenia w/ T retics, BM bx w/ cytoge<strong>net</strong>ics showing hypocellularity• Etiologies: idiopathic ( 1 ⁄2– 2 ⁄3 of cases)stem cell destruction: radiation, chemotherapy, chemicals (eg, benzene)idiosyncratic med rxn (eg, chloramphenicol, NSAIDs, sulfa drugs, gold,carbamazepine, antithyroid)viruses (HHV-6, HIV, EBV, parvovirus B19); also posthepatitis (non A, B, or C)immune disorders (SLE, GVHD post HSCT, thymoma)PNH (see below); Fanconi’s anemia (congenital disorder w/ pancytopenia, macrocyticanemia, c risk of MDS, AML, & SCC of head & neck, and multiple physical anomalies);telomerase (hTERT) mutation (NEJM 2005;352:1413)
- Page 3 and 4:
POCKETNOTEBOOKPocketMEDICINEFourth
- Page 5 and 6:
Contributing AuthorsForewordPreface
- Page 7 and 8:
HIV/AIDS 6-17Tick-Borne Diseases 6-
- Page 9 and 10:
Rajat Gupta, MDInternal Medicine Re
- Page 11 and 12:
FOREWORDTo the 1st EditionIt is wit
- Page 13 and 14:
ELECTROCARDIOGRAPHYApproach (a syst
- Page 15 and 16:
CHEST PAINDisorderUnstableanginaMIP
- Page 17 and 18:
CORONARY ANGIOGRAPHY AND REVASCULAR
- Page 19 and 20:
Likelihood of ACSFeature High Inter
- Page 21 and 22:
STEMIReperfusion• Immediate reper
- Page 23 and 24:
• VT/VF: lido or amio 6-24 h, th
- Page 25 and 26:
PA Catheter WaveformsLocation RA RV
- Page 27 and 28:
Evaluation of the causes of heart f
- Page 29 and 30:
CARDIOMYOPATHIESDiseases with mecha
- Page 31 and 32:
RESTRICTIVE CARDIOMYOPATHY (RCMP)De
- Page 33 and 34:
AORTIC INSUFFICIENCY (AI)Etiology (
- Page 35 and 36:
Clinical manifestations (Lancet 200
- Page 37 and 38:
PERICARDIAL DISEASEGENERAL PRINCIPL
- Page 39 and 40:
CONSTRICTIVE PERICARDITISEtiology
- Page 41 and 42:
• Pharmacologic options (if HTN o
- Page 43 and 44:
ACUTE AORTIC SYNDROMESDefinitions (
- Page 45 and 46:
OnsetRateRhythmP wavemorphologyResp
- Page 47 and 48:
ATRIAL FIBRILLATIONClassification (
- Page 49 and 50:
SYNCOPEDefinition• Symptom of sud
- Page 51 and 52:
INTRACARDIAC DEVICESPacemaker CodeA
- Page 53 and 54:
Pre-operative testing and therapy
- Page 55 and 56:
DYSPNEAPathophysiologyEtiologiesAir
- Page 57 and 58:
Other• Behavior modification: ide
- Page 59 and 60:
CHRONIC OBSTRUCTIVE PULMONARY DISEA
- Page 61 and 62:
HEMOPTYSISDefinition and pathophysi
- Page 63 and 64:
INTERSTITIAL LUNG DISEASEWORKUP OF
- Page 65 and 66:
PLEURAL EFFUSIONPathophysiology•
- Page 67 and 68:
VENOUS THROMBOEMBOLISM (VTE)Definit
- Page 69 and 70:
Risk stratification for Pts with PE
- Page 71 and 72:
• SupportiveOxygen: maintain S aO
- Page 73 and 74:
MECHANICAL VENTILATIONIndications
- Page 75 and 76:
Tailoring the ventilator settings
- Page 77 and 78: SEPSISDefinitionsSystemic2 or more
- Page 79 and 80: ESOPHAGEAL AND GASTRIC DISORDERSDYS
- Page 81 and 82: GASTROINTESTINAL BLEEDINGDefinition
- Page 83 and 84: DIARRHEA, CONSTIPATION, AND ILEUSAC
- Page 85 and 86: Dx: IgA antitissue transglutaminase
- Page 87 and 88: DIVERTICULAR DISEASEDIVERTICULOSISD
- Page 89 and 90: MANAGEMENT (Lancet 2007;369:1641 &
- Page 91 and 92: PANCREATITISPathogenesis• Acinar
- Page 93 and 94: ABNORMAL LIVER TESTSTests of hepato
- Page 95 and 96: HEPATITISVIRALHepatitis A (ssRNA; a
- Page 97 and 98: AUTOIMMUNE HEPATITIS (AIH)Classific
- Page 99 and 100: CIRRHOSISDefinition (Lancet 2008;37
- Page 101 and 102: PrognosisModified Child-Turcotte-Pu
- Page 103 and 104: HEPATIC VASCULAR DISEASEPortal vein
- Page 105 and 106: BILIARY TRACT DISEASECHOLELITHIASIS
- Page 107 and 108: ACID-BASE DISTURBANCESGENERALDefini
- Page 109 and 110: Workup for AG metabolic acidosis•
- Page 111 and 112: Etiologies of Metabolic AlkalosisSa
- Page 113 and 114: Hypovolemic hypotonic hyponatremia
- Page 115 and 116: POLYURIADefinition and pathophysiol
- Page 117 and 118: Treatment• If true potassium defi
- Page 119 and 120: Treatment• Treat underlying disor
- Page 121 and 122: DIALYSISGeneral• Substitutes for
- Page 123 and 124: Treatment• ANCA or anti-GBM: ste
- Page 125 and 126: HEMATURIAEtiologies of HematuriaExt
- Page 127: ANEMIAT in RBC mass: Hct 41% or Hb
- Page 131 and 132: • Infection: splenic infarction S
- Page 133 and 134: PLATELET DISORDERSTHROMBOCYTOPENIA
- Page 135 and 136: • Treatment of type II (NEJM 2006
- Page 137 and 138: HYPERCOAGULABLE STATESSuspect in Pt
- Page 139 and 140: TRANSFUSION THERAPYPacked red blood
- Page 141 and 142: MYELOPROLIFERATIVE NEOPLASMS (MPN)G
- Page 143 and 144: LEUKEMIAACUTE LEUKEMIADefinition•
- Page 145 and 146: Prognosis• CR achieved in 80% of
- Page 147 and 148: LYMPHOMADefinition• Malignant dis
- Page 149 and 150: Consider CNS prophylaxis w/ intrath
- Page 151 and 152: Treatment (NEJM 2004;351:1860; Lanc
- Page 153 and 154: • Sinusoidal obstruction syndrome
- Page 155 and 156: TNM Staging System for NSCLCN stage
- Page 157 and 158: Simplified Staging System for Breas
- Page 159 and 160: COLORECTAL CANCER (CRC)Epidemiology
- Page 161 and 162: PANCREATIC TUMORSPathology and gene
- Page 163 and 164: • Prostate, breast, and lung canc
- Page 165 and 166: PNEUMONIAMicrobiology of PneumoniaC
- Page 167 and 168: FUNGAL INFECTIONSCandida species•
- Page 169 and 170: URINARY TRACT INFECTIONS (UTI)Defin
- Page 171 and 172: Diagnostic studies• Superficial s
- Page 173 and 174: INFECTIONS OF THE NERVOUS SYSTEMACU
- Page 175 and 176: VIRAL ENCEPHALITISDefinition• Vir
- Page 177 and 178: Diagnostic studies• Blood culture
- Page 179 and 180:
TUBERCULOSISEpidemiology• U.S.: 1
- Page 181 and 182:
HIV/AIDSDefinition• AIDS: HIV CD
- Page 183 and 184:
Cutaneous• Seborrheic dermatitis;
- Page 185 and 186:
TICK-BORNE DISEASESDistinguishing F
- Page 187 and 188:
FEVER OF UNKNOWN ORIGIN (FUO)Defini
- Page 189 and 190:
PITUITARY DISORDERSHYPOPITUITARY SY
- Page 191 and 192:
THYROID DISORDERSDiagnostic Studies
- Page 193 and 194:
Clinical manifestations of hyperthy
- Page 195 and 196:
ADRENAL DISORDERSCushing’s Syndro
- Page 197 and 198:
Treatment• Adenoma or carcinoma S
- Page 199 and 200:
CALCIUM DISORDERSLaboratory Finding
- Page 201 and 202:
DIABETES MELLITUSDefinition (Diabet
- Page 203 and 204:
Typical DKA “Flow sheet” SetupV
- Page 205 and 206:
ARTHRITIS—OVERVIEWApproach to pat
- Page 207 and 208:
RHEUMATOID ARTHRITIS (RA)Definition
- Page 209 and 210:
CRYSTAL DEPOSITION ARTHRITIDESGOUTD
- Page 211 and 212:
SERONEGATIVE SPONDYLOARTHRITISGENER
- Page 213 and 214:
INFECTIOUS ARTHRITIS & BURSITISDIAG
- Page 215 and 216:
CONNECTIVE TISSUE DISEASES% Autoant
- Page 217 and 218:
Clinical manifestations• Muscle w
- Page 219 and 220:
SYSTEMIC LUPUS ERYTHEMATOSUS (SLE)M
- Page 221 and 222:
VASCULITISLARGE-VESSEL VASCULITISTa
- Page 223 and 224:
Maintenance: MTX or AZA for 2 yfor
- Page 225 and 226:
CRYOGLOBULINEMIADefinition & Types
- Page 227 and 228:
CHANGE IN MENTAL STATUSDefinitions
- Page 229 and 230:
SEIZURESDefinitions (NEJM 2003;349:
- Page 231 and 232:
ALCOHOL WITHDRAWALPathophysiology
- Page 233 and 234:
Treatment of ischemic stroke (NEJM
- Page 235 and 236:
MYASTHENIA GRAVISDefinition and epi
- Page 237 and 238:
BACK AND SPINAL CORD DISEASEDdx of
- Page 239 and 240:
ACLS ALGORITHMSFigure 10-1 ACLS VF/
- Page 241 and 242:
Figure 10-3 ACLS bradycardia algori
- Page 243 and 244:
DrugClassDoseper kgaverageSedationM
- Page 245 and 246:
FORMULAE AND QUICK REFERENCECARDIOL
- Page 247 and 248:
P KUOsmFigure 10-5 Acetaminophen to
- Page 249 and 250:
Warfarin-heparin overlap therapy•
- Page 251 and 252:
5-NT6-MPa/wAAAAADAbABEABGabnlABPAab
- Page 253 and 254:
FRCFSGSFSHFTIFUOFVCG6PDGBGBMGBSGCAG
- Page 255 and 256:
PIDPIFPIPPKDPMPMFPMHxPMIPMLPMNPMVPM
- Page 257 and 258:
AA-a gradient, 2-18, 10-8abdominal
- Page 259 and 260:
Ddactylitis, 8-7decerebrate posturi
- Page 261 and 262:
Liddle’s syndrome, 4-5, 4-10, 7-8
- Page 263 and 264:
shock, 1-13, 10-4cardiogenic, 1-13s
- Page 265 and 266:
NOTES
- Page 267 and 268:
RadiologyPHOTO INSERT P-11 Normal P
- Page 269 and 270:
PHOTO INSERT P-37 Right middle lobe
- Page 271 and 272:
13 Normal chest CT at level of pulm
- Page 273 and 274:
17 Normal abdomen CT at level of li
- Page 275 and 276:
EchocardiographyVentricular septumR
- Page 277 and 278:
Anterolateralfree wallLeft ventricl
- Page 279 and 280:
Coronary Angiography3LEFT CORONARY
- Page 281:
PHOTO INSERT P-153 CML. 4 CLL.All p