Diagnostic studies• Hyperparathyroidism and malignancy account for 90% of cases of hypercalcemiahyperparathyroidism more likely if asx or chronic hypercalcemiamalignancy more likely if acute or sx; malignancy usually overt or becomes so in mos• Ca, alb, ICa, PTH (may be inappropriately normal in 1 hyperparathyroidism & FHH), PO 4;based on results consider checking PTHrP, 25-(OH)D, 1,25-(OH) 2D, A, U Ca, SPEP,UPEP, ACE, CXR/CT, mammogramAcute Treatment of HypercalcemiaTreatment Onset Duration CommentsNormal saline h during Rx Natriuresis Screnal Ca excretion(4–6 L/d) Furosemide h during Rx Use only if volume overloaded.Bisphosphonates 1–2 d var. Inhibit osteoclasts, useful in malignancy; cautionin renal failure; risk of jaw osteonecrosisCalcitonin h 2–3 d Quickly develop tachyphylaxisGlucocorticoids days days ? Useful in some malig, granulomatous disorders& vitamin D intox.(NEJM 2005;352:373)Treatment of asymptomatic 1 HPT (JCEM 2009;94:335)• Surgery if: age 50 y; serum Ca 1 mg/dL ULN; CrCl 60 mL/min, DEXA T score −2.5• If not yet candidate for surgery: ✓ serum Ca & Cr annually and BMD q1–2yno data yet to support use of bisphosphonates, estrogen, SERMs, or calcimimeticCALCIUM 7-12HYPOCALCEMIAEtiologies of HypocalcemiaCategoryEtiologiesHypoparathyroidism Sporadic; familial (PGA 1, activating Ca-sensing receptor(NEJM 2008;359:391) mutations; see 7-2); iatrogenic (s/p thyroid, cancer surgery,neck irradiation);Wilson’s, hemochromatosis; hypoMg (Tsecretion and effect); activating Ca-sensing receptor autoAbPseudo-Ia and Ib: PTH end organ resistance (∴ c serum PTH)hypoparathyroidism Ia: skeletal abnormalities, short stature, & retardationPseudopseudohypoparathyroidism Ia syndrome but nl Ca & PTHVitamin D deficiency Nutritional/sunlight deprivation; GI disease/fat malabs.; drugsor resistance(anticonvulsants, rifampin, ketoconazole, 5-FU/leucovorin);ge<strong>net</strong>ic (1-hydroxylase,VDR mutations)Chronic renal failure T 1,25-(OH) 2D production, c PO 4 from T clearanceAccelerated <strong>net</strong> bone Postparathyroidectomy, Rx of severe vit D deficiency orFormationPaget’s disease (NEJM 2006;355:593), osteoblastic metastasesCalciumPancreatitis, citrate excess (after blood transfusions),sequestration acute cc PO 4 (ARF, rhabdomyolysis, tumor lysis), bisphosphonatesClinical manifestations• Neurom<strong>usc</strong>ular irritability: perioral paresthesias, cramps, Chvostek’s (tappingfacial nerve S contraction of facial m<strong>usc</strong>les), Trousseau’s (inflation of BP cuff Scarpal spasm), laryngospasm; irritability, depression, psychosis, c ICP, seizures, c QT• Rickets and/or osteomalacia: chronic T vit D STCa, T PO 4 STbone/cartilagemineralization, growth failure, bone pain, m<strong>usc</strong>le weakness• Renal osteodystrophy (T vit D & c PTH in renal failure): osteomalacia (T mineralizationof bone due to T Ca and 1,25-(OH) 2D) & osteitis fibrosa cystica (due to c PTH)Diagnostic studies• Ca, alb, ICa, PTH, 25-(OH)D, 1,25-(OH) 2D (if renal failure or rickets), Cr, Mg, PO 4,A,U CaTreatment (also treat concomitant vitamin D deficiency)• Symptomatic: intravenous Ca gluconate (1–2 g IV over 20 mins) calcitriol (mosteffective in acute hypocalcemia, but takes hrs to work) Mg (50–100 mEq/d)• Asymptomatic and/or chronic: oral Ca (1–3 g/d) & vitamin D (eg, ergocalciferol 50,000 IUPO q wk 8–10 wks). In chronic hypopara., calcitriol is needed, consider also thiazide• Chronic renal failure: phosphate binder(s), oral Ca, calcitriol or analog (calcimimeticmay be needed later to prevent hypercalcemia)
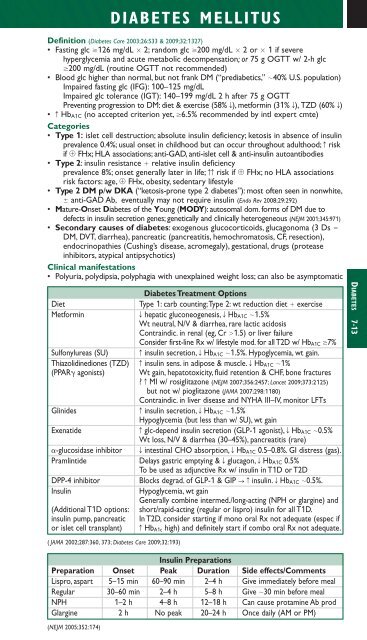
DIABETES MELLITUSDefinition (Diabetes Care 2003;26:S33 & 2009;32:1327)• Fasting glc 126 mg/dL 2; random glc 200 mg/dL 2 or 1 if severehyperglycemia and acute metabolic decompensation;or75 g OGTT w/ 2-h glc200 mg/dL (routine OGTT not recommended)• Blood glc higher than normal, but not frank DM (“prediabetics,” 40% U.S. population)Impaired fasting glc (IFG): 100–125 mg/dLImpaired glc tolerance (IGT): 140–199 mg/dL 2 h after 75 g OGTTPreventing progression to DM: diet & exercise (58% T), metformin (31% T), TZD (60% T)• c Hb A1C (no accepted criterion yet, 6.5% recommended by intl expert cmte)Categories• Type 1: islet cell destruction; absolute insulin deficiency; ketosis in absence of insulinprevalence 0.4%; usual onset in childhood but can occur throughout adulthood; c riskif FHx; HLA associations; anti-GAD, anti-islet cell & anti-insulin autoantibodies• Type 2: insulin resistance relative insulin deficiencyprevalence 8%; onset generally later in life; cc risk if FHx; no HLA associationsrisk factors: age, FHx, obesity, sedentary lifestyle• Type 2 DM p/w DKA (“ketosis-prone type 2 diabetes”): most often seen in nonwhite, anti-GAD Ab, eventually may not require insulin (Endo Rev 2008;29:292)• Mature-Onset Diabetes of the Young (MODY): autosomal dom. forms of DM due todefects in insulin secretion genes; ge<strong>net</strong>ically and clinically heterogeneous (NEJM 2001;345:971)• Secondary causes of diabetes: exogenous glucocorticoids, glucagonoma (3 Ds DM, DVT, diarrhea), pancreatic (pancreatitis, hemochromatosis, CF, resection),endocrinopathies (Cushing’s disease, acromegaly), gestational, drugs (proteaseinhibitors, atypical antipsychotics)Clinical manifestations• Polyuria, polydipsia, polyphagia with unexplained weight loss; can also be asymptomaticDiabetes Treatment OptionsDietType 1: carb counting;Type 2: wt reduction diet exerciseMetforminT hepatic gluconeogenesis, T Hb A1C 1.5%Wt neutral, N/V & diarrhea, rare lactic acidosisContraindic. in renal (eg, Cr 1.5) or liver failureConsider first-line Rx w/ lifestyle mod. for all T2D w/ Hb A1C 7%Sulfonylureas (SU)c insulin secretion, T Hb A1C 1.5%. Hypoglycemia, wt gain.Thiazolidinediones (TZD) c insulin sens. in adipose & m<strong>usc</strong>le. T Hb A1C 1%(PPAR agonists) Wt gain, hepatotoxicity, fluid retention & CHF, bone fractures? c MI w/ rosiglitazone (NEJM 2007;356:2457; Lancet 2009;373:2125)but not w/ pioglitazone (JAMA 2007;298:1180)Contraindic. in liver disease and NYHA III–IV, monitor LFTsGlinidesc insulin secretion, T Hb A1C 1.5%Hypoglycemia (but less than w/ SU), wt gainExenatidec glc-depend insulin secretion (GLP-1 agonist), T Hb A1C 0.5%Wt loss, N/V & diarrhea (30–45%), pancreatitis (rare)-glucosidase inhibitor T intestinal CHO absorption, T Hb A1C 0.5–0.8%. GI distress (gas).Pramlintide Delays gastric emptying & T glucagon, T Hb A1C 0.5%To be used as adjunctive Rx w/ insulin in T1D or T2DDPP-4 inhibitorBlocks degrad. of GLP-1 & GIP Scinsulin. T Hb A1C 0.5%.InsulinHypoglycemia, wt gainGenerally combine intermed./long-acting (NPH or glargine) and(Additional T1D options: short/rapid-acting (regular or lispro) insulin for all T1D.insulin pump, pancreatic In T2D, consider starting if mono oral Rx not adequate (espec ifor islet cell transplant) c Hb A1c high) and definitely start if combo oral Rx not adequate.( JAMA 2002;287:360, 373; Diabetes Care 2009;32:193)DIABETES 7-13Insulin PreparationsPreparation Onset Peak Duration Side effects/CommentsLispro, aspart 5–15 min 60–90 min 2–4 h Give immediately before mealRegular 30–60 min 2–4 h 5–8 h Give 30 min before mealNPH 1–2 h 4–8 h 12–18 h Can cause protamine Ab prodGlargine 2 h No peak 20–24 h Once daily (AM or PM)(NEJM 2005;352:174)
- Page 3 and 4:
POCKETNOTEBOOKPocketMEDICINEFourth
- Page 5 and 6:
Contributing AuthorsForewordPreface
- Page 7 and 8:
HIV/AIDS 6-17Tick-Borne Diseases 6-
- Page 9 and 10:
Rajat Gupta, MDInternal Medicine Re
- Page 11 and 12:
FOREWORDTo the 1st EditionIt is wit
- Page 13 and 14:
ELECTROCARDIOGRAPHYApproach (a syst
- Page 15 and 16:
CHEST PAINDisorderUnstableanginaMIP
- Page 17 and 18:
CORONARY ANGIOGRAPHY AND REVASCULAR
- Page 19 and 20:
Likelihood of ACSFeature High Inter
- Page 21 and 22:
STEMIReperfusion• Immediate reper
- Page 23 and 24:
• VT/VF: lido or amio 6-24 h, th
- Page 25 and 26:
PA Catheter WaveformsLocation RA RV
- Page 27 and 28:
Evaluation of the causes of heart f
- Page 29 and 30:
CARDIOMYOPATHIESDiseases with mecha
- Page 31 and 32:
RESTRICTIVE CARDIOMYOPATHY (RCMP)De
- Page 33 and 34:
AORTIC INSUFFICIENCY (AI)Etiology (
- Page 35 and 36:
Clinical manifestations (Lancet 200
- Page 37 and 38:
PERICARDIAL DISEASEGENERAL PRINCIPL
- Page 39 and 40:
CONSTRICTIVE PERICARDITISEtiology
- Page 41 and 42:
• Pharmacologic options (if HTN o
- Page 43 and 44:
ACUTE AORTIC SYNDROMESDefinitions (
- Page 45 and 46:
OnsetRateRhythmP wavemorphologyResp
- Page 47 and 48:
ATRIAL FIBRILLATIONClassification (
- Page 49 and 50:
SYNCOPEDefinition• Symptom of sud
- Page 51 and 52:
INTRACARDIAC DEVICESPacemaker CodeA
- Page 53 and 54:
Pre-operative testing and therapy
- Page 55 and 56:
DYSPNEAPathophysiologyEtiologiesAir
- Page 57 and 58:
Other• Behavior modification: ide
- Page 59 and 60:
CHRONIC OBSTRUCTIVE PULMONARY DISEA
- Page 61 and 62:
HEMOPTYSISDefinition and pathophysi
- Page 63 and 64:
INTERSTITIAL LUNG DISEASEWORKUP OF
- Page 65 and 66:
PLEURAL EFFUSIONPathophysiology•
- Page 67 and 68:
VENOUS THROMBOEMBOLISM (VTE)Definit
- Page 69 and 70:
Risk stratification for Pts with PE
- Page 71 and 72:
• SupportiveOxygen: maintain S aO
- Page 73 and 74:
MECHANICAL VENTILATIONIndications
- Page 75 and 76:
Tailoring the ventilator settings
- Page 77 and 78:
SEPSISDefinitionsSystemic2 or more
- Page 79 and 80:
ESOPHAGEAL AND GASTRIC DISORDERSDYS
- Page 81 and 82:
GASTROINTESTINAL BLEEDINGDefinition
- Page 83 and 84:
DIARRHEA, CONSTIPATION, AND ILEUSAC
- Page 85 and 86:
Dx: IgA antitissue transglutaminase
- Page 87 and 88:
DIVERTICULAR DISEASEDIVERTICULOSISD
- Page 89 and 90:
MANAGEMENT (Lancet 2007;369:1641 &
- Page 91 and 92:
PANCREATITISPathogenesis• Acinar
- Page 93 and 94:
ABNORMAL LIVER TESTSTests of hepato
- Page 95 and 96:
HEPATITISVIRALHepatitis A (ssRNA; a
- Page 97 and 98:
AUTOIMMUNE HEPATITIS (AIH)Classific
- Page 99 and 100:
CIRRHOSISDefinition (Lancet 2008;37
- Page 101 and 102:
PrognosisModified Child-Turcotte-Pu
- Page 103 and 104:
HEPATIC VASCULAR DISEASEPortal vein
- Page 105 and 106:
BILIARY TRACT DISEASECHOLELITHIASIS
- Page 107 and 108:
ACID-BASE DISTURBANCESGENERALDefini
- Page 109 and 110:
Workup for AG metabolic acidosis•
- Page 111 and 112:
Etiologies of Metabolic AlkalosisSa
- Page 113 and 114:
Hypovolemic hypotonic hyponatremia
- Page 115 and 116:
POLYURIADefinition and pathophysiol
- Page 117 and 118:
Treatment• If true potassium defi
- Page 119 and 120:
Treatment• Treat underlying disor
- Page 121 and 122:
DIALYSISGeneral• Substitutes for
- Page 123 and 124:
Treatment• ANCA or anti-GBM: ste
- Page 125 and 126:
HEMATURIAEtiologies of HematuriaExt
- Page 127 and 128:
ANEMIAT in RBC mass: Hct 41% or Hb
- Page 129 and 130:
MACROCYTIC ANEMIASincludes megalobl
- Page 131 and 132:
• Infection: splenic infarction S
- Page 133 and 134:
PLATELET DISORDERSTHROMBOCYTOPENIA
- Page 135 and 136:
• Treatment of type II (NEJM 2006
- Page 137 and 138:
HYPERCOAGULABLE STATESSuspect in Pt
- Page 139 and 140:
TRANSFUSION THERAPYPacked red blood
- Page 141 and 142:
MYELOPROLIFERATIVE NEOPLASMS (MPN)G
- Page 143 and 144:
LEUKEMIAACUTE LEUKEMIADefinition•
- Page 145 and 146:
Prognosis• CR achieved in 80% of
- Page 147 and 148:
LYMPHOMADefinition• Malignant dis
- Page 149 and 150: Consider CNS prophylaxis w/ intrath
- Page 151 and 152: Treatment (NEJM 2004;351:1860; Lanc
- Page 153 and 154: • Sinusoidal obstruction syndrome
- Page 155 and 156: TNM Staging System for NSCLCN stage
- Page 157 and 158: Simplified Staging System for Breas
- Page 159 and 160: COLORECTAL CANCER (CRC)Epidemiology
- Page 161 and 162: PANCREATIC TUMORSPathology and gene
- Page 163 and 164: • Prostate, breast, and lung canc
- Page 165 and 166: PNEUMONIAMicrobiology of PneumoniaC
- Page 167 and 168: FUNGAL INFECTIONSCandida species•
- Page 169 and 170: URINARY TRACT INFECTIONS (UTI)Defin
- Page 171 and 172: Diagnostic studies• Superficial s
- Page 173 and 174: INFECTIONS OF THE NERVOUS SYSTEMACU
- Page 175 and 176: VIRAL ENCEPHALITISDefinition• Vir
- Page 177 and 178: Diagnostic studies• Blood culture
- Page 179 and 180: TUBERCULOSISEpidemiology• U.S.: 1
- Page 181 and 182: HIV/AIDSDefinition• AIDS: HIV CD
- Page 183 and 184: Cutaneous• Seborrheic dermatitis;
- Page 185 and 186: TICK-BORNE DISEASESDistinguishing F
- Page 187 and 188: FEVER OF UNKNOWN ORIGIN (FUO)Defini
- Page 189 and 190: PITUITARY DISORDERSHYPOPITUITARY SY
- Page 191 and 192: THYROID DISORDERSDiagnostic Studies
- Page 193 and 194: Clinical manifestations of hyperthy
- Page 195 and 196: ADRENAL DISORDERSCushing’s Syndro
- Page 197 and 198: Treatment• Adenoma or carcinoma S
- Page 199: CALCIUM DISORDERSLaboratory Finding
- Page 203 and 204: Typical DKA “Flow sheet” SetupV
- Page 205 and 206: ARTHRITIS—OVERVIEWApproach to pat
- Page 207 and 208: RHEUMATOID ARTHRITIS (RA)Definition
- Page 209 and 210: CRYSTAL DEPOSITION ARTHRITIDESGOUTD
- Page 211 and 212: SERONEGATIVE SPONDYLOARTHRITISGENER
- Page 213 and 214: INFECTIOUS ARTHRITIS & BURSITISDIAG
- Page 215 and 216: CONNECTIVE TISSUE DISEASES% Autoant
- Page 217 and 218: Clinical manifestations• Muscle w
- Page 219 and 220: SYSTEMIC LUPUS ERYTHEMATOSUS (SLE)M
- Page 221 and 222: VASCULITISLARGE-VESSEL VASCULITISTa
- Page 223 and 224: Maintenance: MTX or AZA for 2 yfor
- Page 225 and 226: CRYOGLOBULINEMIADefinition & Types
- Page 227 and 228: CHANGE IN MENTAL STATUSDefinitions
- Page 229 and 230: SEIZURESDefinitions (NEJM 2003;349:
- Page 231 and 232: ALCOHOL WITHDRAWALPathophysiology
- Page 233 and 234: Treatment of ischemic stroke (NEJM
- Page 235 and 236: MYASTHENIA GRAVISDefinition and epi
- Page 237 and 238: BACK AND SPINAL CORD DISEASEDdx of
- Page 239 and 240: ACLS ALGORITHMSFigure 10-1 ACLS VF/
- Page 241 and 242: Figure 10-3 ACLS bradycardia algori
- Page 243 and 244: DrugClassDoseper kgaverageSedationM
- Page 245 and 246: FORMULAE AND QUICK REFERENCECARDIOL
- Page 247 and 248: P KUOsmFigure 10-5 Acetaminophen to
- Page 249 and 250: Warfarin-heparin overlap therapy•
- Page 251 and 252:
5-NT6-MPa/wAAAAADAbABEABGabnlABPAab
- Page 253 and 254:
FRCFSGSFSHFTIFUOFVCG6PDGBGBMGBSGCAG
- Page 255 and 256:
PIDPIFPIPPKDPMPMFPMHxPMIPMLPMNPMVPM
- Page 257 and 258:
AA-a gradient, 2-18, 10-8abdominal
- Page 259 and 260:
Ddactylitis, 8-7decerebrate posturi
- Page 261 and 262:
Liddle’s syndrome, 4-5, 4-10, 7-8
- Page 263 and 264:
shock, 1-13, 10-4cardiogenic, 1-13s
- Page 265 and 266:
NOTES
- Page 267 and 268:
RadiologyPHOTO INSERT P-11 Normal P
- Page 269 and 270:
PHOTO INSERT P-37 Right middle lobe
- Page 271 and 272:
13 Normal chest CT at level of pulm
- Page 273 and 274:
17 Normal abdomen CT at level of li
- Page 275 and 276:
EchocardiographyVentricular septumR
- Page 277 and 278:
Anterolateralfree wallLeft ventricl
- Page 279 and 280:
Coronary Angiography3LEFT CORONARY
- Page 281:
PHOTO INSERT P-153 CML. 4 CLL.All p