PHT 2-16PULMONARY HYPERTENSION (PHT)PA mean pressure 25 mm Hg at rest or 30 mm Hg with exertionPathobiology (NEJM 2004;35:1655)• Smooth m<strong>usc</strong>le & endothelial cell proliferation: c VEGF, ET-1, 5-HT; T PGI 2, NO,VIP;mutations in bone morphogenic protein receptor 2 (BMPR2; gene involved in prolif. &apoptosis) seen in 50% familial and 26% sporadic cases of PPH (NEJM 2001;345:319)• Imbalance between vasoconstrictors and vasodilatorsc vasoconstrictors: thromboxane A 2 (TXA 2), serotonin (5-HT), endothelin-1 (ET-1)T vasodilators: prostacyclin (PGI 2), nitric oxide (NO), vasoactive peptide (VIP)• In situ thrombosis: c TXA 2, 5-HT, PAI-1; T PGI 2, NO,VIP, tissue plasminogen activatorEtiologies of Pulmonary Hypertension (Revised WHO Classification)Pulmonary arterial • Idiopathic (IPAH): mean age of onset 36 y ( older than );HTN (PAH): 2:1, usually mild c in PAP• Familial (FPAH)• Associated conditions (APAH)Connective tissue disorders: CREST, SLE, MCTD, RA, PM, SjögrenCongenital LSR shunts:ASD,VSD, PDAPortopulmonary HTN (? 2 vasoactive substances not filtered inESLD; Z hepatopulmonary syndrome)HIV; drugs & toxins: anorexic agents, rapeseed oil, L-tryptophanOther: thyroid dis., glycogen storage dis., Gaucher disease, HHT,hemoglobinopathies, chronic myeloprolif d/o, splenectomy• Pulmonary veno-occlusive disease: ? 2 chemo, BMT; orthopnea,CHF, pl eff, nl PCWP; art vasodil. worsen CHF (AJRCCM 2000;162:1964)• Pulmonary capillary hemangiomatosisLeft heart disease • Left atrial or ventricular (diastolic or systolic) dysfunction• Left-sided valvular heart disease (eg, MS/MR)Lung diseases and/ • COPD • Alveolar hypoventilation (eg, NM disease)or chronic • ILD • Chronic hypoxemia (eg, high altitude)hypoxemia • Sleep apnea • Developmental abnormalitiesChronic thrombotic • Obstruction of proximal or distal pulmonary arteriesor embolic disease • Nonthrombotic emboli (tumor, foreign body, parasites)Miscellaneous • Sarcoidosis, histiocytosis X, lymphangiomatosis, schistosomiasis• Compression of pulm vessels (adenopathy, tumor, fibrosingmediastinitis)(Circulation 2009;28:119:2250)Clinical manifestations• Dyspnea, exertional syncope (hypoxia, T CO), exertional chest pain (RV ischemia)• Symptoms of R-sided CHF (eg, peripheral edema, RUQ fullness, abdominal distention)Physical exam• PHT: prominent P 2, R-sided S 4, RV heave, PA tap & flow murmur, PR (Graham Steell),TR• RV failure: c JVP, hepatomegaly, peripheral edemaDiagnostic studies & workup (Circ 2009;119:2250)• IPAH yearly incidence 1–2 per million, ∴ r/o 2 causes• CXR and high-resolution chest CT: dilatation & pruning of pulmonary arteries,enlargement of RA and RV; r/o parenchymal lung disease• ECG: RAD, RBBB, RAE (“P pulmonale”), RVH (Se 55%, Sp 70%)• PFTs: T D LCO, mild restrictive pattern; r/o obstructive and restrictive lung disease• ABG & polysomnography: T P aO 2 and S aO 2 (especially w/ exertion), T P aCO 2, c A-agradient; r/o hypoventilation and OSA• TTE: c RVSP (but over or under by 10 mm Hg in 1 ⁄2 of PHT Pts; AJRCCM 2009;179:615),flattened (“D”) septum,TR, PR; r/o LV dysfxn, MV disease, and congenital heart disease• RHC: c RA, RV, & PA pressures, nl PCWP (unless due to L-sided heart disease),c transpulm gradient (PAP-PCWP 12–15, but can be nl if due to LV or valvular dis.),c PVR, T CO; r/o c L-sided pressures shunt• CTA (large/med vessel),V/Q scan (small vessel), pulmonary angiogram: r/o PE andchronic thromboembolic disease• Vasculitis labs: ANA (commonly in PPH), RF, anti-Scl-70, anti-centromere, ESR• LFTs & HIV: r/o portopulmonary and HIV-associated PAH• 6-min walk test (6MWT) or cardiopulmonary exercise testing to establish fxnl capacityTreatment (NEJM 2004;351:1425; JIM 2005;258:199; Circ 2009;119:2250)• Principles1) prevent and reverse vasoactive substance imbalance and vascular remodeling2) prevent RV failure: T wall stress (T PVR, PAP, RV diam); ensure adeq. systemic DBP
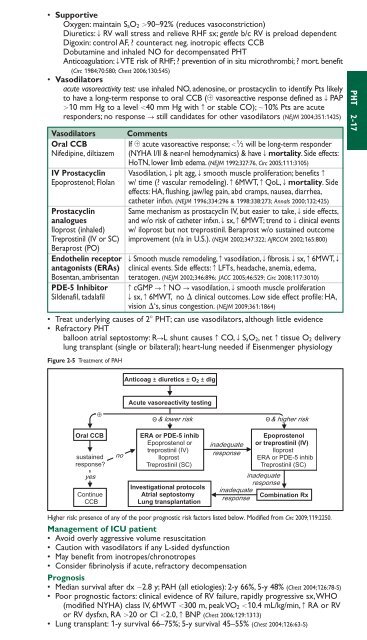
• SupportiveOxygen: maintain S aO 2 90–92% (reduces vasoconstriction)Diuretics: T RV wall stress and relieve RHF sx; gentle b/c RV is preload dependentDigoxin: control AF, ? counteract neg. inotropic effects CCBDobutamine and inhaled NO for decompensated PHTAnticoagulation: TVTE risk of RHF; ? prevention of in situ microthrombi; ? mort. benefit(Circ 1984;70:580; Chest 2006;130:545)• Vasodilatorsacute vasoreactivity test: use inhaled NO, adenosine, or prostacyclin to identify Pts likelyto have a long-term response to oral CCB ( vasoreactive response defined as T PAP10 mm Hg to a level 40 mm Hg with c or stable CO); 10% Pts are acuteresponders; no response S still candidates for other vasodilators (NEJM 2004;351:1425)Vasodilators CommentsOral CCBIf acute vasoreactive response; 1 ⁄2 will be long-term responderNifedipine, diltiazem (NYHA I/II & near-nl hemodynamics) & have T mortality. Side effects:HoTN, lower limb edema. (NEJM 1992;327:76, Circ 2005;111:3105)IV Prostacyclin Vasodilation, T plt agg, T smooth m<strong>usc</strong>le proliferation; benefits cEpoprostenol; Flolan w/ time (? vascular remodeling). c 6MWT, c QoL, T mortality. Sideeffects: HA, flushing, jaw/leg pain, abd cramps, nausea, diarrhea,catheter infxn. (NEJM 1996;334:296 & 1998:338:273; Annals 2000;132:425)Prostacyclin Same mechanism as prostacyclin IV, but easier to take, T side effects,analoguesand w/o risk of catheter infxn. T sx, c 6MWT; trend to T clinical eventsIloprost (inhaled) w/ iloprost but not treprostinil. Beraprost w/o sustained outcomeTreprostinil (IV or SC) improvement (n/a in U.S.). (NEJM 2002;347:322; AJRCCM 2002;165:800)Beraprost (PO)Endothelin receptor T Smooth m<strong>usc</strong>le remodeling, c vasodilation, T fibrosis. T sx, c 6MWT, Tantagonists (ERAs) clinical events. Side effects: c LFTs, headache, anemia, edema,Bosentan, ambrisentan teratogen. (NEJM 2002;346:896; JACC 2005;46:529; Circ 2008;117:3010)PDE-5 InhibitorSildenafil, tadalafilc cGMP ScNO S vasodilation, T smooth m<strong>usc</strong>le proliferationT sx, c 6MWT, no clinical outcomes. Low side effect profile: HA,vision ‘s, sinus congestion. (NEJM 2009;361:1864)• Treat underlying causes of 2 PHT; can use vasodilators, although little evidence• Refractory PHTballoon atrial septostomy: RSL shunt causes c CO, T S aO 2, <strong>net</strong> c tissue O 2 deliverylung transplant (single or bilateral); heart-lung needed if Eisenmenger physiologyFigure 2-5 Treatment of PAHPHT 2-17Anticoag ± diuretics ± O2 ± dig⊕Oral CCBsustainedresponse?yesContinueCCBnoAcute vasoreactivity testing& lower risk & higher riskERA or PDE-5 inhibEpoprostenol ortreprostinil (IV)IloprostTreprostinil (SC)Investigational protocolsAtrial septostomyLung transplantationinadequateresponseEpoprostenolor treprostinil (IV)IloprostERA or PDE-5 inhibTreprostinil (SC)inadequateresponseinadequateresponseCombination RxHigher risk: presence of any of the poor prognostic risk factors listed below. Modified from Circ 2009;119:2250.Management of ICU patient• Avoid overly aggressive volume res<strong>usc</strong>itation• Caution with vasodilators if any L-sided dysfunction• May benefit from inotropes/chronotropes• Consider fibrinolysis if acute, refractory decompensationPrognosis• Median survival after dx 2.8 y; PAH (all etiologies): 2-y 66%, 5-y 48% (Chest 2004;126:78-S)• Poor prognostic factors: clinical evidence of RV failure, rapidly progressive sx,WHO(modified NYHA) class IV, 6MWT 300 m, peak VO 2 10.4 mL/kg/min, c RA or RVor RV dysfxn, RA 20 or CI 2.0, c BNP (Chest 2006;129:1313)• Lung transplant: 1-y survival 66–75%; 5-y survival 45–55% (Chest 2004;126:63-S)
- Page 3 and 4:
POCKETNOTEBOOKPocketMEDICINEFourth
- Page 5 and 6:
Contributing AuthorsForewordPreface
- Page 7 and 8:
HIV/AIDS 6-17Tick-Borne Diseases 6-
- Page 9 and 10:
Rajat Gupta, MDInternal Medicine Re
- Page 11 and 12:
FOREWORDTo the 1st EditionIt is wit
- Page 13 and 14:
ELECTROCARDIOGRAPHYApproach (a syst
- Page 15 and 16:
CHEST PAINDisorderUnstableanginaMIP
- Page 17 and 18:
CORONARY ANGIOGRAPHY AND REVASCULAR
- Page 19 and 20: Likelihood of ACSFeature High Inter
- Page 21 and 22: STEMIReperfusion• Immediate reper
- Page 23 and 24: • VT/VF: lido or amio 6-24 h, th
- Page 25 and 26: PA Catheter WaveformsLocation RA RV
- Page 27 and 28: Evaluation of the causes of heart f
- Page 29 and 30: CARDIOMYOPATHIESDiseases with mecha
- Page 31 and 32: RESTRICTIVE CARDIOMYOPATHY (RCMP)De
- Page 33 and 34: AORTIC INSUFFICIENCY (AI)Etiology (
- Page 35 and 36: Clinical manifestations (Lancet 200
- Page 37 and 38: PERICARDIAL DISEASEGENERAL PRINCIPL
- Page 39 and 40: CONSTRICTIVE PERICARDITISEtiology
- Page 41 and 42: • Pharmacologic options (if HTN o
- Page 43 and 44: ACUTE AORTIC SYNDROMESDefinitions (
- Page 45 and 46: OnsetRateRhythmP wavemorphologyResp
- Page 47 and 48: ATRIAL FIBRILLATIONClassification (
- Page 49 and 50: SYNCOPEDefinition• Symptom of sud
- Page 51 and 52: INTRACARDIAC DEVICESPacemaker CodeA
- Page 53 and 54: Pre-operative testing and therapy
- Page 55 and 56: DYSPNEAPathophysiologyEtiologiesAir
- Page 57 and 58: Other• Behavior modification: ide
- Page 59 and 60: CHRONIC OBSTRUCTIVE PULMONARY DISEA
- Page 61 and 62: HEMOPTYSISDefinition and pathophysi
- Page 63 and 64: INTERSTITIAL LUNG DISEASEWORKUP OF
- Page 65 and 66: PLEURAL EFFUSIONPathophysiology•
- Page 67 and 68: VENOUS THROMBOEMBOLISM (VTE)Definit
- Page 69: Risk stratification for Pts with PE
- Page 73 and 74: MECHANICAL VENTILATIONIndications
- Page 75 and 76: Tailoring the ventilator settings
- Page 77 and 78: SEPSISDefinitionsSystemic2 or more
- Page 79 and 80: ESOPHAGEAL AND GASTRIC DISORDERSDYS
- Page 81 and 82: GASTROINTESTINAL BLEEDINGDefinition
- Page 83 and 84: DIARRHEA, CONSTIPATION, AND ILEUSAC
- Page 85 and 86: Dx: IgA antitissue transglutaminase
- Page 87 and 88: DIVERTICULAR DISEASEDIVERTICULOSISD
- Page 89 and 90: MANAGEMENT (Lancet 2007;369:1641 &
- Page 91 and 92: PANCREATITISPathogenesis• Acinar
- Page 93 and 94: ABNORMAL LIVER TESTSTests of hepato
- Page 95 and 96: HEPATITISVIRALHepatitis A (ssRNA; a
- Page 97 and 98: AUTOIMMUNE HEPATITIS (AIH)Classific
- Page 99 and 100: CIRRHOSISDefinition (Lancet 2008;37
- Page 101 and 102: PrognosisModified Child-Turcotte-Pu
- Page 103 and 104: HEPATIC VASCULAR DISEASEPortal vein
- Page 105 and 106: BILIARY TRACT DISEASECHOLELITHIASIS
- Page 107 and 108: ACID-BASE DISTURBANCESGENERALDefini
- Page 109 and 110: Workup for AG metabolic acidosis•
- Page 111 and 112: Etiologies of Metabolic AlkalosisSa
- Page 113 and 114: Hypovolemic hypotonic hyponatremia
- Page 115 and 116: POLYURIADefinition and pathophysiol
- Page 117 and 118: Treatment• If true potassium defi
- Page 119 and 120: Treatment• Treat underlying disor
- Page 121 and 122:
DIALYSISGeneral• Substitutes for
- Page 123 and 124:
Treatment• ANCA or anti-GBM: ste
- Page 125 and 126:
HEMATURIAEtiologies of HematuriaExt
- Page 127 and 128:
ANEMIAT in RBC mass: Hct 41% or Hb
- Page 129 and 130:
MACROCYTIC ANEMIASincludes megalobl
- Page 131 and 132:
• Infection: splenic infarction S
- Page 133 and 134:
PLATELET DISORDERSTHROMBOCYTOPENIA
- Page 135 and 136:
• Treatment of type II (NEJM 2006
- Page 137 and 138:
HYPERCOAGULABLE STATESSuspect in Pt
- Page 139 and 140:
TRANSFUSION THERAPYPacked red blood
- Page 141 and 142:
MYELOPROLIFERATIVE NEOPLASMS (MPN)G
- Page 143 and 144:
LEUKEMIAACUTE LEUKEMIADefinition•
- Page 145 and 146:
Prognosis• CR achieved in 80% of
- Page 147 and 148:
LYMPHOMADefinition• Malignant dis
- Page 149 and 150:
Consider CNS prophylaxis w/ intrath
- Page 151 and 152:
Treatment (NEJM 2004;351:1860; Lanc
- Page 153 and 154:
• Sinusoidal obstruction syndrome
- Page 155 and 156:
TNM Staging System for NSCLCN stage
- Page 157 and 158:
Simplified Staging System for Breas
- Page 159 and 160:
COLORECTAL CANCER (CRC)Epidemiology
- Page 161 and 162:
PANCREATIC TUMORSPathology and gene
- Page 163 and 164:
• Prostate, breast, and lung canc
- Page 165 and 166:
PNEUMONIAMicrobiology of PneumoniaC
- Page 167 and 168:
FUNGAL INFECTIONSCandida species•
- Page 169 and 170:
URINARY TRACT INFECTIONS (UTI)Defin
- Page 171 and 172:
Diagnostic studies• Superficial s
- Page 173 and 174:
INFECTIONS OF THE NERVOUS SYSTEMACU
- Page 175 and 176:
VIRAL ENCEPHALITISDefinition• Vir
- Page 177 and 178:
Diagnostic studies• Blood culture
- Page 179 and 180:
TUBERCULOSISEpidemiology• U.S.: 1
- Page 181 and 182:
HIV/AIDSDefinition• AIDS: HIV CD
- Page 183 and 184:
Cutaneous• Seborrheic dermatitis;
- Page 185 and 186:
TICK-BORNE DISEASESDistinguishing F
- Page 187 and 188:
FEVER OF UNKNOWN ORIGIN (FUO)Defini
- Page 189 and 190:
PITUITARY DISORDERSHYPOPITUITARY SY
- Page 191 and 192:
THYROID DISORDERSDiagnostic Studies
- Page 193 and 194:
Clinical manifestations of hyperthy
- Page 195 and 196:
ADRENAL DISORDERSCushing’s Syndro
- Page 197 and 198:
Treatment• Adenoma or carcinoma S
- Page 199 and 200:
CALCIUM DISORDERSLaboratory Finding
- Page 201 and 202:
DIABETES MELLITUSDefinition (Diabet
- Page 203 and 204:
Typical DKA “Flow sheet” SetupV
- Page 205 and 206:
ARTHRITIS—OVERVIEWApproach to pat
- Page 207 and 208:
RHEUMATOID ARTHRITIS (RA)Definition
- Page 209 and 210:
CRYSTAL DEPOSITION ARTHRITIDESGOUTD
- Page 211 and 212:
SERONEGATIVE SPONDYLOARTHRITISGENER
- Page 213 and 214:
INFECTIOUS ARTHRITIS & BURSITISDIAG
- Page 215 and 216:
CONNECTIVE TISSUE DISEASES% Autoant
- Page 217 and 218:
Clinical manifestations• Muscle w
- Page 219 and 220:
SYSTEMIC LUPUS ERYTHEMATOSUS (SLE)M
- Page 221 and 222:
VASCULITISLARGE-VESSEL VASCULITISTa
- Page 223 and 224:
Maintenance: MTX or AZA for 2 yfor
- Page 225 and 226:
CRYOGLOBULINEMIADefinition & Types
- Page 227 and 228:
CHANGE IN MENTAL STATUSDefinitions
- Page 229 and 230:
SEIZURESDefinitions (NEJM 2003;349:
- Page 231 and 232:
ALCOHOL WITHDRAWALPathophysiology
- Page 233 and 234:
Treatment of ischemic stroke (NEJM
- Page 235 and 236:
MYASTHENIA GRAVISDefinition and epi
- Page 237 and 238:
BACK AND SPINAL CORD DISEASEDdx of
- Page 239 and 240:
ACLS ALGORITHMSFigure 10-1 ACLS VF/
- Page 241 and 242:
Figure 10-3 ACLS bradycardia algori
- Page 243 and 244:
DrugClassDoseper kgaverageSedationM
- Page 245 and 246:
FORMULAE AND QUICK REFERENCECARDIOL
- Page 247 and 248:
P KUOsmFigure 10-5 Acetaminophen to
- Page 249 and 250:
Warfarin-heparin overlap therapy•
- Page 251 and 252:
5-NT6-MPa/wAAAAADAbABEABGabnlABPAab
- Page 253 and 254:
FRCFSGSFSHFTIFUOFVCG6PDGBGBMGBSGCAG
- Page 255 and 256:
PIDPIFPIPPKDPMPMFPMHxPMIPMLPMNPMVPM
- Page 257 and 258:
AA-a gradient, 2-18, 10-8abdominal
- Page 259 and 260:
Ddactylitis, 8-7decerebrate posturi
- Page 261 and 262:
Liddle’s syndrome, 4-5, 4-10, 7-8
- Page 263 and 264:
shock, 1-13, 10-4cardiogenic, 1-13s
- Page 265 and 266:
NOTES
- Page 267 and 268:
RadiologyPHOTO INSERT P-11 Normal P
- Page 269 and 270:
PHOTO INSERT P-37 Right middle lobe
- Page 271 and 272:
13 Normal chest CT at level of pulm
- Page 273 and 274:
17 Normal abdomen CT at level of li
- Page 275 and 276:
EchocardiographyVentricular septumR
- Page 277 and 278:
Anterolateralfree wallLeft ventricl
- Page 279 and 280:
Coronary Angiography3LEFT CORONARY
- Page 281:
PHOTO INSERT P-153 CML. 4 CLL.All p