


You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
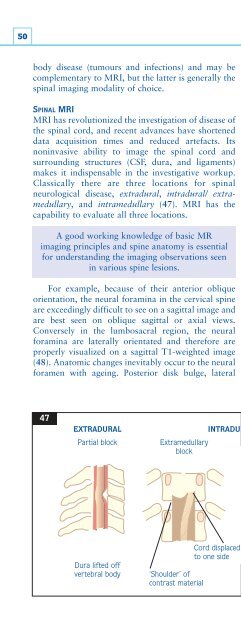
50body disease (tumours and infections) and may becomplementary to MRI, but the latter is generally thespinal imaging modality of choice.SPINAL MRIMRI has revolutionized the investigation of disease ofthe spinal cord, and recent advances have shorteneddata acquisition times and reduced artefacts. Itsnoninvasive ability to image the spinal cord andsurrounding structures (CSF, dura, and ligaments)makes it indispensable in the investigative workup.Classically there are three locations for spinalneurological disease, extradural, intradural/ extramedullary,and intramedullary (47). MRI has thecapability to evaluate all three locations.A good working knowledge of basic MRimaging principles and spine anatomy is essentialfor understanding the imaging observations seenin various spine lesions.For example, because of their anterior obliqueorientation, the neural foramina in the cervical spineare exceedingly difficult to see on a sagittal image andare best seen on oblique sagittal or axial views.Conversely in the lumbosacral region, the neuralforamina are laterally orientated and therefore areproperly visualized on a sagittal T1-weighted image(48). Anatomic changes inevitably occur to the neuralforamen with ageing. Posterior disk bulge, lateralherniated disk, together with vertebral bodyosteophytes can encroach on the neural foramen andits contents. Although MRI is poor in showing densenormal cortical bone, it shows infiltrative/infectivedisease well. Contrast-medium enhanced imaging canhelp differentiate tumours, inflammation, and activedemyelinating diseases.A common mistake is failure to order views thatdisplay the likely site(s) of the lesion. In most cases,careful history and examination will decide which ofcervical, thoracic, or lumbosacral levels are to beimaged. However, this is not always possible and ‘fullspinal imaging’ should then be requested. Somedisease processes can be multilevel (multiple sclerosis[MS]) and, on occasion, the common (lumbar discdisease) and the rare (thoracic meningioma) maycoexist. In any patient with a spinal cord syndrome ofunknown cause, the clinician must consider thepossibility of a lesion at the level of the foramenmagnum, a level that is neither spinal nor cranial andconsequently is often overlooked. Imaging hereshould pay particular attention to the possibility ofmalformations (Chiari malformations) and thelocation of the odontoid process (rheumatoidarthritis). A benign tumour of the foramen magnumsuch as meningioma can be confused with MS ordegenerative cord diseases and, prior to correctdiagnosis, progressive disability passes beyond thepoint of reversibility.47EXTRADURALINTRADURALPartial block Extramedullary Intramedullaryblockblock47 Illustration of extradural andintradural (extramedullary andintramedullary) spaces.Cord displacedto one sideDura lifted offContrast material isvertebral body ‘Shoulder’ of splayed around thecontrast materialdilated cord













