


You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
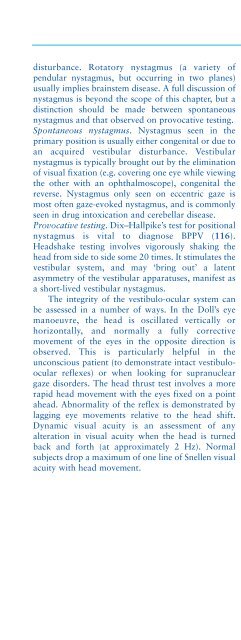
Disorders of special senses 141disturbance. Rotatory nystagmus (a variety ofpendular nystagmus, but occurring in two planes)usually implies brainstem disease. A full discussion ofnystagmus is beyond the scope of this chapter, but adistinction should be made between spontaneousnystagmus and that observed on provocative testing.Spontaneous nystagmus. Nystagmus seen in theprimary position is usually either congenital or due toan acquired vestibular disturbance. Vestibularnystagmus is typically brought out by the eliminationof visual fixation (e.g. covering one eye while viewingthe other with an ophthalmoscope), congenital thereverse. Nystagmus only seen on eccentric gaze ismost often gaze-evoked nystagmus, and is commonlyseen in drug intoxication and cerebellar disease.Provocative testing. Dix–Hallpike’s test for positionalnystagmus is vital to diagnose BPPV (116).Headshake testing involves vigorously shaking thehead from side to side some 20 times. It stimulates thevestibular system, and may ‘bring out’ a latentasymmetry of the vestibular apparatuses, manifest asa short-lived vestibular nystagmus.The integrity of the vestibulo-ocular system canbe assessed in a number of ways. In the Doll’s eyemanoeuvre, the head is oscillated vertically orhorizontally, and normally a fully correctivemovement of the eyes in the opposite direction isobserved. This is particularly helpful in theunconscious patient (to demonstrate intact vestibuloocularreflexes) or when looking for supranucleargaze disorders. The head thrust test involves a morerapid head movement with the eyes fixed on a pointahead. Abnormality of the reflex is demonstrated bylagging eye movements relative to the head shift.Dynamic visual acuity is an assessment of anyalteration in visual acuity when the head is turnedback and forth (at approximately 2 Hz). Normalsubjects drop a maximum of one line of Snellen visualacuity with head movement.ab116116 Diagram to illustrate the Dix–Hallpike positional test. Thepatient is positioned so that when lying flat, the head extendsover the end of the table. With the patient sitting upright, thephysician turns and holds the patient's head at 45° to the side(right or left). The patient is then rapidly laid down with thehead extended over the edge of the table (a, b). The eyes arecarefully observed for the development of positionalnystagmus, which is usually not immediate. Severe vertiginoussymptoms usually accompany a positive test. Finally, thepatient should be sat upright and the eyes observed fornystagmus.













