


You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
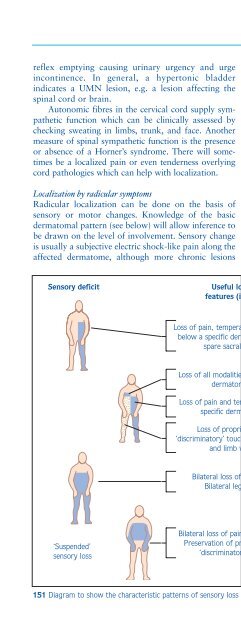
Disorders of sensation207reflex emptying causing urinary urgency and urgeincontinence. In general, a hypertonic bladderindicates a UMN lesion, e.g. a lesion affecting thespinal cord or brain.Autonomic fibres in the cervical cord supply sympatheticfunction which can be clinically assessed bychecking sweating in limbs, trunk, and face. Anothermeasure of spinal sympathetic function is the presenceor absence of a Horner’s syndrome. There will sometimesbe a localized pain or even tenderness overlyingcord pathologies which can help with localization.Localization by radicular symptomsRadicular localization can be done on the basis ofsensory or motor changes. Knowledge of the basicdermatomal pattern (see below) will allow inference tobe drawn on the level of involvement. Sensory changeis usually a subjective electric shock-like pain along theaffected dermatome, although more chronic lesionscan lead to numbness in the affected area. Motorchanges will usually involve reduction or loss of therelevant reflexes on the affected side (Table 55).Differentiation of radicular symptoms fromperipheral nerve-related symptoms can only be donewhen there is a knowledge of the characteristicpatterns of innervation of each of the peripheralnerves and the functions supplied by each spinal root.This can be difficult, however, and somecharacteristic pitfalls are listed (Table 56). Directpressure on the sacral roots by a lumbar or sacrallesion causes a LMN bladder, with loss of sensationof fullness and an atonic overfilling bladder.Lesion anatomical localizationThe extent and pattern of involvement of the spinalcord in disease may result in characteristic patterns ofdeficit, which can give further clues to the nature ofthe pathological process (151).Sensory deficit Useful localizing Lesion sitefeatures (if present)CONTRALATERALSPINOTHALAMICTRACT LESIONLoss of pain, temperature and light touchbelow a specific dermatome level (mayspare sacral sensation)Loss of all modalities at one or severaldermatome levelsLoss of pain and temperature below aspecific dermatome level(Partialspinothalamictract lesion)BROWN-SÉQUARD SYNDROME151Loss of proprioception and‘discriminatory’ touch up to similar leveland limb weakness(Partial cord lesion)Bilateral loss of all modalities.Bilateral leg weaknessCOMPLETE CORD LESION‘Suspended’sensory lossBilateral loss of pain and temperature.Preservation of proprioception and‘discriminatory’ sensationCENTRAL CORD LESION151 Diagram to show the characteristic patterns of sensory loss in various spinal cord lesions.













