


You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
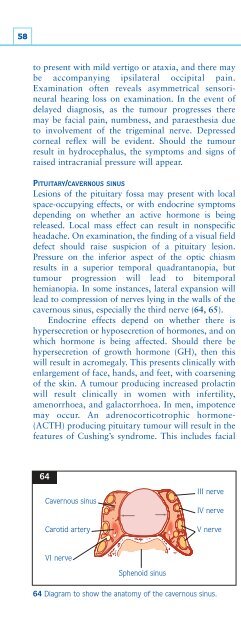
58to present with mild vertigo or ataxia, and there maybe accompanying ipsilateral occipital pain.Examination often reveals asymmetrical sensorineuralhearing loss on examination. In the event ofdelayed diagnosis, as the tumour progresses theremay be facial pain, numbness, and paraesthesia dueto involvement of the trigeminal nerve. Depressedcorneal reflex will be evident. Should the tumourresult in hydrocephalus, the symptoms and signs ofraised intracranial pressure will appear.PITUITARY/CAVERNOUS SINUSLesions of the pituitary fossa may present with localspace-occupying effects, or with endocrine symptomsdepending on whether an active hormone is beingreleased. Local mass effect can result in nonspecificheadache. On examination, the finding of a visual fielddefect should raise suspicion of a pituitary lesion.Pressure on the inferior aspect of the optic chiasmresults in a superior temporal quadrantanopia, buttumour progression will lead to bitemporalhemianopia. In some instances, lateral expansion willlead to compression of nerves lying in the walls of thecavernous sinus, especially the third nerve (64, 65).Endocrine effects depend on whether there ishypersecretion or hyposecretion of hormones, and onwhich hormone is being affected. Should there behypersecretion of growth hormone (GH), then thiswill result in acromegaly. This presents clinically withenlargement of face, hands, and feet, with coarseningof the skin. A tumour producing increased prolactinwill result clinically in women with infertility,amenorrhoea, and galactorrhoea. In men, impotencemay occur. An adrenocorticotrophic hormone-(ACTH) producing pituitary tumour will result in thefeatures of Cushing’s syndrome. This includes facialmooning, hirsutism, central obesity, and muscleweakness.Investigation of lesions affecting the pituitary orcavernous sinus primarily involves neuroimaging andtests of endocrine function. The imaging modality ofchoice for investigating pituitary lesions is MRI (66).This gives excellent anatomical detail, and can showwhether there is suprasellar extension and whetheradjacent structures such as the walls of the cavernoussinus are involved. Given the close proximity of thepituitary to the optic chiasm, it is important to testvisual fields as a means of monitoring involvement ofvisual pathways. This is best done at the bedside byassessing peripheral visual fields using a red hatpin. Itmay be supplemented by more detailed Goldmannperimetry, available in ophthalmology clinics.Hypersecretion may be diagnosed by measuringblood levels of the relevant hormone. While manyendocrine presentations of pituitary tumours are dueto hypersecretion, it is also possible for pituitarylesions to present clinically with signs of impairmentof pituitary secretion. This may present clinically asadult GH deficiency syndrome (weight gain, loss oflibido, fatigue), muscle weakness and fatigue, or withthe symptoms of hypothyroidism. Low levels ofpituitary hormone in the presence of low target glandhormones confirm hyposecretion. This can be further6564Cavernous sinusCarotid arteryIII nerveIV nerveV nerveVI nerveSphenoid sinus64 Diagram to show the anatomy of the cavernous sinus.65 Computed tomography scan of cavernous sinus thrombosis.













