


You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
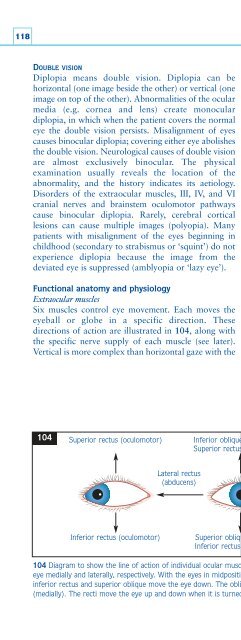
118DOUBLE VISIONDiplopia means double vision. Diplopia can behorizontal (one image beside the other) or vertical (oneimage on top of the other). Abnormalities of the ocularmedia (e.g. cornea and lens) create monoculardiplopia, in which when the patient covers the normaleye the double vision persists. Misalignment of eyescauses binocular diplopia; covering either eye abolishesthe double vision. Neurological causes of double visionare almost exclusively binocular. The physicalexamination usually reveals the location of theabnormality, and the history indicates its aetiology.Disorders of the extraocular muscles, III, IV, and VIcranial nerves and brainstem oculomotor pathwayscause binocular diplopia. Rarely, cerebral corticallesions can cause multiple images (polyopia). Manypatients with misalignment of the eyes beginning inchildhood (secondary to strabismus or ‘squint’) do notexperience diplopia because the image from thedeviated eye is suppressed (amblyopia or ‘lazy eye’).Functional anatomy and physiologyExtraocular musclesSix muscles control eye movement. Each moves theeyeball or globe in a specific direction. Thesedirections of action are illustrated in 104, along withthe specific nerve supply of each muscle (see later).Vertical is more complex than horizontal gaze with theoblique muscles moving the eye up and down when itis turned in (ADduction) and the recti moving the eyeup and down when it is turned out (ABduction). If anextraocular muscle is weak, movement of the eye inthe direction of the muscle’s action will be impaired,and the patient will see double when looking in thatdirection, because conjugate eye movement has beendisrupted. The false image lies outermost and comesfrom the underacting eye (105). Extraocular musclesmay be affected directly by muscle (e.g. myositis) orneuromuscular junction (NMJ) disorders (e.g.myasthenia gravis) that make the muscles weak orrestricted.OrbitThe optic nerve enters the orbit through the opticforamen, alongside the ophthalmic artery. The nervesthat supply ocular movement (see below) enter theorbit through the superior orbital fissure. Orbitalapex anatomy is illustrated in 106. Masses (whichmay be inflammatory, infective, or neoplastic) in theorbit may displace the globe (causing proptosis orforward displacement of the globe), maymechanically interfere with the extraocular muscles,or may compress the nerves supplying ocularmovement, so causing cranial nerve palsy. They mayalso cause visual loss, due to interference with theoptic nerve at the orbital apex.104 Superior rectus (oculomotor) Inferior oblique (oculomotor) Inferior oblique (oculomotor)Superior rectus (oculomotor)Lateral rectus(abducens)Medial rectus(oculomotor)Inferior rectus (oculomotor) Superior oblique (trochlear) Superior oblique (trochlear)Inferior rectus (oculomotor)104 Diagram to show the line of action of individual ocular muscles and their nerve supply. Medial and lateral rectus move theeye medially and laterally, respectively. With the eyes in midposition, superior rectus and inferior oblique move the eye up, andinferior rectus and superior oblique move the eye down. The oblique muscles move the eye up and down when it is turned in(medially). The recti move the eye up and down when it is turned out (laterally).













