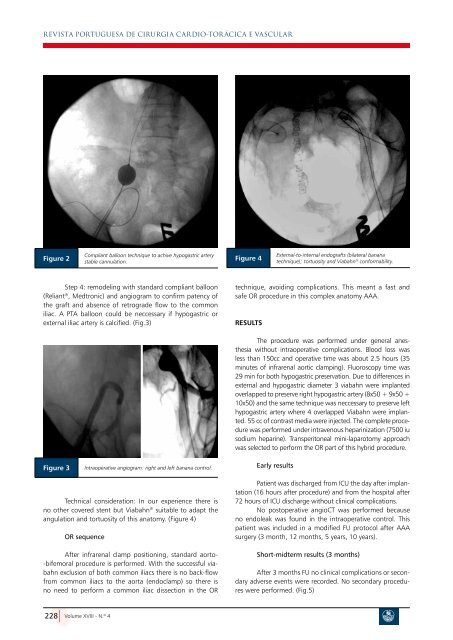
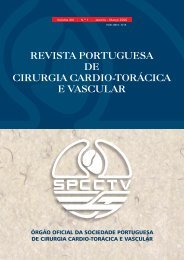
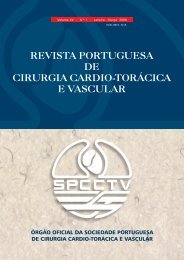
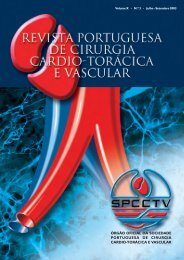
REVISTA PORTUGUESA DE CIRURGIA CARDIO-TOR áCICA E VASCULARFigure 2Compliant balloon technique to achive hypogastric arterystable cannulation.Figure 4External-to-internal endografts (bilateral bananatechnique); tortuosity and Viabahn ® conformability.Step 4: remodeling with standard compliant balloon(Reliant ® , Medtronic) and angiogram to confirm patency ofthe graft and absence of retrograde flow to the commoniliac. A PTA balloon could be neccessary if hypogastric orexternal iliac artery is calcified. (Fig.3)technique, avoiding complications. This meant a fast andsafe OR procedure in this complex anatomy AAA.ResultsFigure 3Intraoperative angiogram: right and left banana control.The procedure was performed under general anesthesiawithout intraoperative complications. Blood loss wasless than 150cc and operative time was about 2.5 hours (35minutes of infrarenal aortic clamping). Fluoroscopy time was29 min for both hypogastric preservation. Due to differences inexternal and hypogastric diameter 3 viabahn were implantedoverlapped to preserve right hypogastric artery (8x50 + 9x50 +10x50) and the same technique was neccessary to preserve lefthypogastric artery where 4 overlapped Viabahn were implanted.55 cc of contrast media were injected. The complete procedurewas performed under intravenous heparinization (7500 iusodium heparine). Transperitoneal mini-laparotomy approachwas selected to perform the OR part of this hybrid procedure.Early resultsTechnical consideration: In our experience there isno other covered stent but Viabahn ® suitable to ada<strong>pt</strong> theangulation and tortuosity of this anatomy. (Figure 4)OR sequenceAfter infrarenal clamp positioning, standard aorto--bifemoral procedure is performed. With the successful viabahnexclusion of both common iliacs there is no back-flowfrom common iliacs to the aorta (endoclamp) so there isno need to perform a common iliac dissection in the ORPatient was discharged from ICU the day after implantation(16 hours after procedure) and from the hospital after72 hours of ICU discharge without clinical complications.No postoperative angioCT was performed becauseno endoleak was found in the intraoperative control. Thispatient was included in a modified FU protocol after AAAsurgery (3 month, 12 months, 5 years, 10 years).Short-midterm results (3 months)After 3 months FU no clinical complications or secondaryadverse events were recorded. No secondary procedureswere performed. (Fig.5)228 Volume XVIII - N.º 4
REVISTA PORTUGUESA DE CIRURGIA CARDIO-TOR áCICA E VASCULARThis hybrid strategy, seems to be a safe o<strong>pt</strong>ion tothe surgical hypogastric preservation with by-pass grafting,avoiding potential complications of this technique.There is no strong evidence supporting this techniqueand all the literature avaliable is related mainly to EVARwith aorto-uni-iliac (AUI) devices 6,17-21 .In our experience, we´ve performed this technique in5 AUI cases before with 100% technical success and 100%patency after 2 years FU; so we are quite confident in midand log-term results with the hybrid approach.EVAR resources like Z-BIS® iliac branch techniqueor Sandwich-graft technique are promising treatments butthere is not evidence enogh to support the standard use ofthese techniques in low-risk patients.Once the technique is stablished, to preserve asmuch hypogastric arteries as possible, seemed to be feasibleand easy, so actually we are willing to apply this techniqueto unilateral cases too.ConclusionsFigure 5Discusion3 months AngioCT control.The hypogastric artery preservation still controversialin EVAR procedures but as previously was demonstrated bythe open repair, the complication with intentional occlusionof both hypogastric arteries is higher and it seems to be adecuatetrying to preserve at least one if possible 1-5,14,16-21 .The operative risk in aorto-iliac aneurysm disease isrelated to iliac complications 1-3,6 .This hybrid Banana technique seems to be a safe andfeasible treatment to aorto-iliac aneurysm preserving thehypogastric artery.This hybrid technique could be a good approachto hypogastric preservation in low risk and young patients,reducing potencial complications of hypogastric arteryocclusion or complete open repair technique with hypogastricby-pass revascularization.The specific features of Viabahn® covered stentmakes this graft ideal to perform this technique. This deviceconforms easily to the complex anatomy of the retrogradehypogastric approach making feasible aorto-iliac aneurysmrepair with hypogastric Banana technique preservation.BIBLIOGRAFIA1. Richardson JW, Greenfield LJ. Natural history and managementof iliac aneurysms. J Vasc Surg. 1988;8:165-71.2. Krupsky WC, Selzman CH, Floridia R, Strecker PK, Nehler MR,White-hill TA. Contemporary Management of isolated iliacaneurysms. J Vasc. Surg. 1998;28:1-11;discussion 11-3.3. Arko FR, Lee WA, Hill BB, Fogarty TJ, Zarins CK. Hypogastricartery bypass to preserve pelvic circulation: improved outcomeafter endovascular abdominal aortic aneurysm repair. J VascSurg. 2004 Feb:39(2):404-8.4. Dix FP, Titi M, Al-Khaffaf H. The isolated internal artery aneurysm,a review. Eur J Vasc Endovasc Surg 2005;30:119-29.5. Dorigo W, Pulli R, Troisi N, Alessi-Innocenti A, Pratessi G, AzasL, et al. The treatment of isolated iliaca artery aneurysm inpatients with non-aneurysmal aorta. Eur J Vasc. EndovascularSurg; 35:585-9.6. Patel NV, Long GW, Cheema ZF, Rimar K, Brown OW. Openvs endovascular repair of isolated iliac artery aneurysms: a12-year experience. J Vasc Surg. 2009;49:1147-53.7. Karthikesalingam A, Hinchliffe RJ, Holt PJ, Boyle JR, Loftus IM,Thompson MM: Endovascular aneurysm repair with preservationof the internal iliac artery using the iliac branch graftdevice. Eur J Vasc Endovascular Surg. 2010 Mar; 39(3):285-94.8. Ziegler P, Avgerinos ED, Umscheid T, Perdikides T, Erz K, SteiterWJ: Branched iliac bifurcation: 6 years experience with endovascularpreservation of internal iliac artery flow. J Vasc Surg.2007 Aug;46(2):204-10.9. Malina M, Resch T, Sonesson B: EVAR and complex anatomy:an update on fenestrated and branched stent grafts. ScandinavianJournal of Surgery 2008;97:195-204.10. Ohrlander T, Sonesson B, Ivancev K, Resch T, Dias N, MalinaM: The chimney graft: a technique for preserving or rescuingaortic branch vessels in stent-graft sealing zones. J EndovascTher. 2008;15(4):427-32.11. Allaqaband S, Jan MF, Bajwa T: “The chimney-graft”-a simpletechnique for endovascular repair of complex juxtarenal abdominalaortic aneurysm in noo<strong>pt</strong>ion patients. Catheter CardiovascInterv. 2010;75(7):1111-5.12. Allaqaband S, Kumar A, Bajwa T: A novel technique of aortomonoiliacAAA repair in patients with a single patent iliac artery: a“stent-graft sandwich”. J Endovasc Ther 2004;11(5):550-2.13. Donas KP, Torsello G, Austermann M, Schwindt A, Troisi N,Pitoulias GA: Use of abdominal chimney grafts is feasible andsafe: short-term results. J Endovasc Ther 2010;17(5):589-93.14. Mosquera NJ, Rodriguez-Feijoo G, Carballo-Fernandez C,Volume XVIII - N.º 4229