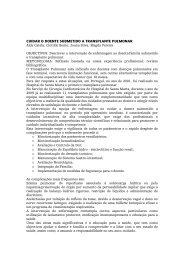
REVISTA PORTUGUESA DE CIRURGIA CARDIO-TOR áCICA E VASCULARFigura 7Angiografia 3D mostrando procedimento cirúrgicorealizado, um ano após a operação.atenuar-se com o tempo, sendo a taxa de complicações comnecessidade de segunda intervenção superior para o tratamentoendovascular.Apesar da sua aceitação crescente, sobretudo emdoentes de alto risco, Harris et al. 3 mostraram que a taxade conversão após tratamento endovascular para a cirurgiaconvencional não é desprezível, representando um riscocumulativo de 2,1% ao ano. Por sua vez Verzini et al. 4 reportaram9 % de conversões aos 6 anos. Os endoleaks tipo Ie III, assim como a migração prótesica, são os principaisresponsáveis pela conversão numa sub-análise do estudoEUROSTAR, realizada por Fransen et al. 5 que revelou aindaque a rotura do aneurisma após terapêutica endovascularestá associada a uma mortalidade de 62%.Assim, a cirurgia convencional assume importânciacrescente no tratamento após insucesso do tratamentoendovascular, contudo a mesma não é isenta de mortalidade,atingindo os 24,4% 3 .O caso clinico por nós apresentado tornou-se aindamais desafiante pela forma de apresentação da rotura, comfistula artério-venosa ilíaca de alto débito.As fístulas artério-venosas de alto débito são decorrentesem 80 6 a 90% 7 da rotura de aneurismas para osistema venoso, este evento apresenta uma baixa taxa deincidência ocorrendo em menos de 1% de todos os aneurismase em 3 a 6% dos aneurismas rotos sintomáticos. 6,7O seu diagnóstico depende do reconhecimento de umconjunto de sinais e sintomas assim como da execução deexames complementares de diagnóstico. Classicamentepodem manifestar-se com dor lombar intensa, dispneia,presença de massa abdominal pulsátil, auscultação desopro abdominal, frémito palpável e hipertensão venosaregional manifestando-se por edema uni ou bilateral dosmembros, podendo ser confundida com trombose venosaprofunda. A clinica pode ser fruste ou ausente, sendo odiagnóstico por vezes só efectuado através dos examescomplementares de diagnóstico, angiografia, ecodopplerou angio-TC.A apresentação abru<strong>pt</strong>a causada pela rotura doaneurisma com instalação súbita de fístula artério-venosa dealto débito e insuficiência cardíaca direita, está associada auma mortalidade descrita entre 21 e 55% para os aneurismasaórticos e de 5 a 10% para os aneurismas ilíacos, sendoo seu tratamento cirúrgico urgente 6 .O tratamento do aneurisma em rotura pós intervençãoendovascular é sempre desafiante, quer pela instabilidadehemodinâmica, quer pela reacção inflamatória aórticaresultante do corpo estranho prótesico 8 . Estão descritas técnicasde resgate pós EVAR com a remoção total ou parcial daendoprótese 9,10 e posterior interposição aorto-bifemoral ouaorto-femoral, sendo que a opção de remover a totalidadeda prótese implica sempre uma clampagem mais proximal,os autores defendem que a clampagem sobre o corpo relativamenterígido da endoprótese pode induzir na paredeaórtica lesão iatrogénica dificilmente reparável, não sendoassim recomendada 9,10 . O bypass extra-anatómico prévio,axilo-femoral ou bifemoral, e posterior laqueação aórticaapós a emergência das artérias renais pode ainda constituiroutra opção de tratamento, sobretudo em casos de infecçãoprótesica 11 .ConclusãoOs autores concluem que a reparação “in situ” porcirurgia convencional do aneurisma ilíaco em rotura apóstratamento endovascular prévio com fístula artério-venosade alto débito estabelecida é possível com bons resultados,requerendo no entanto, elevada diferenciação técnica.A terapêutica cirúrgica deverá ser emergente e realizadaantes do estabelecimento de insuficiência cardíacadireita, uma vez que a morbilidade e mortalidade são superioresapós o seu aparecimento, sendo considerada factor demau prognóstico.A endoprótese representa um corpo estranho nointerior do lúmen aórtico que condiciona reacção inflamatóriaperi-aórtica, fragiliza a parede arterial e causa dificuldadesno isolamento e clampagem da mesma, dificultandoa tarefa do cirurgião.Sempre que tecnicamente possível, a clampagemdeverá ser próximal à fixação da endoprótese. A anastomoseaórtica deverá ser efectuada entre o corpo da endoprótese(preservando a fixação e o segmento proximal desta) e omaterial protésico a implantar, uma vez que a sua remoçãopoderá causar lesão iatrogénica da parede arterial irreparável,excepção feita à infecção protésica, onde toda a endoprótesedeverá ser removida após a realização um bypassextra-anatómico.A fístula artério-venosa ilíaca contribuiu, em nossaopinião, para a forma pouco habitual de apresentação clínicade rotura do aneurisma ilíaco, constituindo um desafiodiagnóstico e terapêutico.234 Volume XVIII - N.º 4
REVISTA PORTUGUESA DE CIRURGIA CARDIO-TOR áCICA E VASCULARBIBLIOGRAFIA1. Parodi JC, Palmaz JC, Barone HD. Transfemoral intraluminalgraft implantation for abdominal aortic aneurysms. Ann VascSurg. 1991; 5:491-496.2. The United Kingdom EVAR Trial Investigators. Endovascularversus Open Repair of Abdominal Aortic Aneurysm. N Engl JMed. 2010; 362:1863-1871.3. Harris PL, Vallabhaneni SR, Desgranges P, et al. Incidence andrisk factors of late ru<strong>pt</strong>ure, conversion, and death after endovascularrepair of infrarenal aortic aneurysms: the EUROSTARexperience. European Collaborators on Stent/graft techniquesfor aortic aneurysm repair. J Vasc Surg. 2000; 32:739–749.4. Verzini F, Cao P, De Rango P, et al. Conversion to open repair afterendografting for abdominal aortic aneurysm: cause, incidenceand results. Eur J Vasc Endovasc Surg. 2006; 31:136–142.5. G. A. J. Fransen, S. R. Vallabhaneni, C. J. van Marrewijk, R.J. F. Laheij, P. L. Harris, J. Buth. Ru<strong>pt</strong>ure of Infra-renal AorticAneurysm after Endovascular Repair: A Series from EUROSTARRegistry. Eur J Vasc Endovasc Surg. 2003; 26: 487–493.6. Brewster DC, Cambria RP, Moncure AC, Darling RC, LaMuragliaGM, Geller SC, Abbott WM. Aortocaval and iliac arteriovenousfistulas: recognition and treatment. J Vasc Surg. 1991;13(2):253–264.7. Tsolakis JA, Papadoulas S, Kakkos SK, Skroubis G, Siablis D,Androulakis JA. Aortocaval fistula in ru<strong>pt</strong>ured aneurysms. EurJ Vasc Endovasc Surg. 1999; 17:390–393.8. Lyden SP, McNamara JM, Sternbach Y, et al. Technical considerationsfor late removal of aortic endografts. J Vasc Surg.2002; 36:674–678.9. Gambardella I, Blair PH, McKinley A, et al. Successful delayedsecondary open conversion after endovascular repair usingpartial explantation technique: a single-center experience. AnnVasc Surg. 2010; 24:646–654.10. Kelso RL, Lyden SP, Butler B, et al. Late conversion of aorticstent grafts. J Vasc Surg. 2009; 49:589–595.11. Lee CW, Chung SW, Kim JW, Kim S, Bae MJ, Kim CW. Ru<strong>pt</strong>uredAbdominal Aortic Aneurysm after Endovascular AorticAneurysm Repair. Korean J Thorac Cardiovasc Surg. 2011 Feb;44(1):68-71.Volume XVIII - N.º 4235