Ch. 54 – Biliary System
Ch. 54 – Biliary System
Ch. 54 – Biliary System

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
1558 Section X Abdomen<br />
patients tend to have recurring symptoms, usually<br />
repeated episodes of biliary colic. 10 Over a 20-year period,<br />
two thirds of asymptomatic patients with gallstones<br />
remain symptom-free.<br />
<strong>Ch</strong>ronic Calculous <strong>Ch</strong>olecystitis<br />
Ongoing infl ammation with recurrent episodes of biliary<br />
colic or pain from cystic duct obstruction is referred to<br />
as chronic cholecystitis. About two thirds of patients with<br />
gallstone disease present with these repeated attacks.<br />
Although the pathologic changes in the gallbladder can<br />
vary, repeated attacks, scarring, and a nonfunctioning<br />
gallbladder are the rule. Histologically, chronic cholecystitis<br />
is characterized by an increase in subepithelial and<br />
subserosal fi brosis and a mononuclear cell infi ltrate.<br />
Clinical Presentation<br />
The primary symptom of chronic cholecystitis or symptomatic<br />
cholelithiasis is pain, often referred to as biliary<br />
colic (see earlier section, Abdominal Pain). The pain is<br />
constant and usually lasts 1 to 5 hours. The attacks<br />
usually last for more than 1 hour but subsides by 24<br />
hours; if pain persists longer than 1 day, acute cholecystitis<br />
is likely the underlying etiology. The attacks are discrete<br />
and severe enough that patients can accurately<br />
recall and number them. Other symptoms such as nausea<br />
and vomiting often accompany each episode, and bloating<br />
and belching may also be present in 50% of cases.<br />
Fever and jaundice are rare with simple biliary colic.<br />
Patients without symptoms, about two thirds of patients<br />
with gallstones, develop symptoms infrequently and<br />
complications at an even lower rate. In most cases, treatment<br />
is not necessary in these asymptomatic patients.<br />
Patients with gallstones but an atypical presentation<br />
should have other causes of right upper quadrant pain<br />
ruled out such as peptic ulcer disease, pneumonia, renal<br />
calculi, liver disease, hernia, refl ux, or angina.<br />
The physical examination and liver function tests are<br />
usually completely normal in patients with chronic cholecystitis,<br />
particularly if they are pain-free. During an<br />
episode of biliary colic, mild right upper quadrant tenderness<br />
may also be present.<br />
Diagnosis<br />
The diagnosis of symptomatic gallstones or chronic calculous<br />
cholecystitis relies on the clinical presentation and<br />
evidence of gallstones on diagnostic imaging. The presence<br />
of symptoms, typically biliary colic, attributable to<br />
the gallbladder is necessary to consider any treatment for<br />
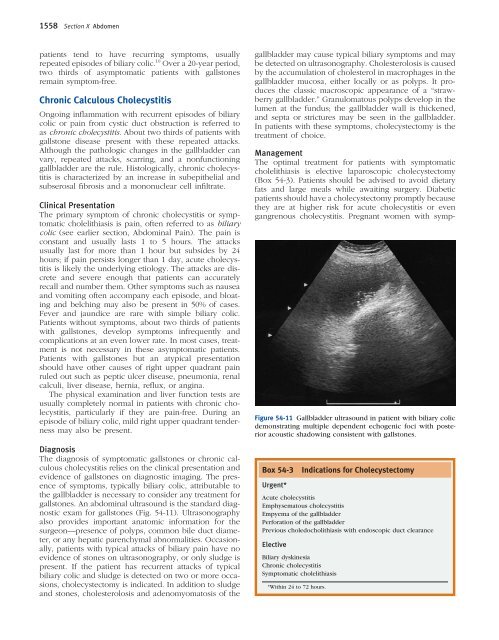
gallstones. An abdominal ultrasound is the standard diagnostic<br />
exam for gallstones (Fig. <strong>54</strong>-11). Ultrasonography<br />
also provides important anatomic information for the<br />
surgeon—presence of polyps, common bile duct diameter,<br />
or any hepatic parenchymal abnormalities. Occasionally,<br />
patients with typical attacks of biliary pain have no<br />
evidence of stones on ultrasonography, or only sludge is<br />
present. If the patient has recurrent attacks of typical<br />
biliary colic and sludge is detected on two or more occasions,<br />
cholecystectomy is indicated. In addition to sludge<br />
and stones, cholesterolosis and adenomyomatosis of the<br />
gallbladder may cause typical biliary symptoms and may<br />
be detected on ultrasonography. <strong>Ch</strong>olesterolosis is caused<br />
by the accumulation of cholesterol in macrophages in the<br />
gallbladder mucosa, either locally or as polyps. It produces<br />
the classic macroscopic appearance of a “strawberry<br />
gallbladder.” Granulomatous polyps develop in the<br />
lumen at the fundus; the gallbladder wall is thickened,<br />
and septa or strictures may be seen in the gallbladder.<br />
In patients with these symptoms, cholecystectomy is the<br />
treatment of choice.<br />
Management<br />
The optimal treatment for patients with symptomatic<br />
cholelithiasis is elective laparoscopic cholecystectomy<br />
(Box <strong>54</strong>-3). Patients should be advised to avoid dietary<br />
fats and large meals while awaiting surgery. Diabetic<br />
patients should have a cholecystectomy promptly because<br />
they are at higher risk for acute cholecystitis or even<br />
gangrenous cholecystitis. Pregnant women with symp-<br />
Figure <strong>54</strong>-11 Gallbladder ultrasound in patient with biliary colic<br />
demonstrating multiple dependent echogenic foci with posterior<br />
acoustic shadowing consistent with gallstones.<br />
Box <strong>54</strong>-3 Indications for <strong>Ch</strong>olecystectomy<br />
Urgent*<br />
Acute cholecystitis<br />
Emphysematous cholecystitis<br />
Empyema of the gallbladder<br />
Perforation of the gallbladder<br />
Previous choledocholithiasis with endoscopic duct clearance<br />
Elective<br />
<strong>Biliary</strong> dyskinesia<br />
<strong>Ch</strong>ronic cholecystitis<br />
Symptomatic cholelithiasis<br />
*Within 24 to 72 hours.