Ch. 54 – Biliary System
Ch. 54 – Biliary System
Ch. 54 – Biliary System

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
1578 Section X Abdomen<br />
abdominal mass. Only 10% of patients present with this<br />
triad. Adults have a slightly different presentation (abdominal<br />
pain and jaundice) than children because of a higher<br />
incidence of bile calculi or sludge and pancreatic-biliary<br />
ductal malformation.<br />
Severe hepatobiliary complications may result from<br />
long-standing biliary cysts if left untreated. Portal hypertension<br />
may develop as a result of portal vein compression<br />
by the adjacent cyst or cirrhosis secondary to<br />
long-term biliary obstruction. Some patients may present<br />
with variceal hemorrhage as an initial manifestation. Very<br />
rarely, patients may present with bilious ascites and peritonitis<br />
as a result of rupture of a choledochal cyst, and<br />
pseudocysts may appear surrounding the common bile<br />
duct. Those patients also have a high incidence of developing<br />
sludge, cholelithiasis, or choledocholithiasis and<br />
have commonly had a prior cholecystectomy.<br />
The incidence of carcinoma (bile duct, hepatic, or<br />
gallbladder in origin) in the choledochal cyst ranges from<br />
2.5% to 26%, which is well above the rate of less than<br />
1% for the general population. Many patients have biliary<br />
cancer at the time of initial presentation. <strong>Ch</strong>ronic infl ammation<br />
caused by bile stagnation has been suggested as<br />
a possible mechanism for the development of cancer by<br />
causing metaplasia of the epithelium of the cystic wall.<br />
Laboratory evaluation may demonstrate liver dysfunction<br />
in 60% of adult patients but is not specifi c. The<br />
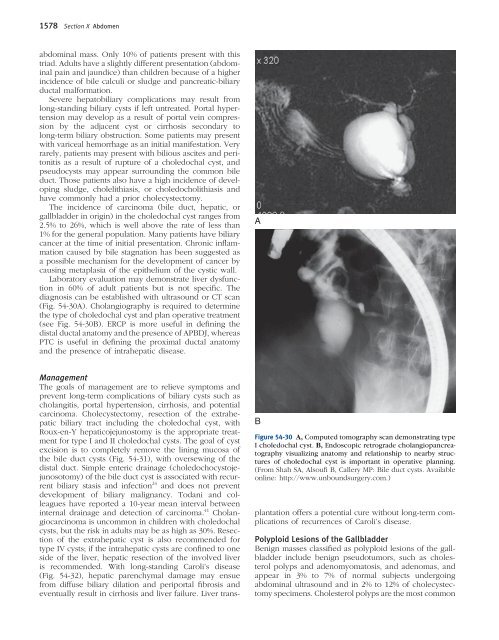
diagnosis can be established with ultrasound or CT scan<br />
(Fig. <strong>54</strong>-30A). <strong>Ch</strong>olangiography is required to determine<br />
the type of choledochal cyst and plan operative treatment<br />
(see Fig. <strong>54</strong>-30B). ERCP is more useful in defi ning the<br />
distal ductal anatomy and the presence of APBDJ, whereas<br />
PTC is useful in defi ning the proximal ductal anatomy<br />
and the presence of intrahepatic disease.<br />
Management<br />
The goals of management are to relieve symptoms and<br />
prevent long-term complications of biliary cysts such as<br />
cholangitis, portal hypertension, cirrhosis, and potential<br />
carcinoma. <strong>Ch</strong>olecystectomy, resection of the extrahepatic<br />
biliary tract including the choledochal cyst, with<br />
Roux-en-Y hepaticojejunostomy is the appropriate treatment<br />
for type I and II choledochal cysts. The goal of cyst<br />
excision is to completely remove the lining mucosa of<br />
the bile duct cysts (Fig. <strong>54</strong>-31), with oversewing of the<br />
distal duct. Simple enteric drainage (choledochocystojejunosotomy)<br />
of the bile duct cyst is associated with recurrent<br />
biliary stasis and infection 24 and does not prevent<br />
development of biliary malignancy. Todani and colleagues<br />
have reported a 10-year mean interval between<br />
internal drainage and detection of carcinoma. 41 <strong>Ch</strong>olangiocarcinoma<br />
is uncommon in children with choledochal<br />
cysts, but the risk in adults may be as high as 30%. Resection<br />
of the extrahepatic cyst is also recommended for<br />
type IV cysts; if the intrahepatic cysts are confi ned to one<br />
side of the liver, hepatic resection of the involved liver<br />
is recommended. With long-standing Caroli’s disease<br />
(Fig. <strong>54</strong>-32), hepatic parenchymal damage may ensue<br />
from diffuse biliary dilation and periportal fi brosis and<br />
eventually result in cirrhosis and liver failure. Liver trans-<br />
A<br />
B<br />
Figure <strong>54</strong>-30 A, Computed tomography scan demonstrating type<br />
I choledochal cyst. B, Endoscopic retrograde cholangiopancreatography<br />
visualizing anatomy and relationship to nearby structures<br />
of choledochal cyst is important in operative planning.<br />
(From Shah SA, Alsoufi B, Callery MP: Bile duct cysts. Available<br />
online: http://www.unboundsurgery.com.)<br />
plantation offers a potential cure without long-term complications<br />
of recurrences of Caroli’s disease.<br />
Polyploid Lesions of the Gallbladder<br />
Benign masses classifi ed as polyploid lesions of the gallbladder<br />
include benign pseudotumors, such as cholesterol<br />
polyps and adenomyomatosis, and adenomas, and<br />
appear in 3% to 7% of normal subjects undergoing<br />
abdominal ultrasound and in 2% to 12% of cholecystectomy<br />
specimens. <strong>Ch</strong>olesterol polyps are the most common