Ch. 54 – Biliary System
Ch. 54 – Biliary System
Ch. 54 – Biliary System

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
1582 Section X Abdomen<br />
Survival<br />
1.0<br />
0.8<br />
0.6<br />
0.4<br />
0.2<br />
0.0<br />
0 12 24 36 48 60<br />
Months<br />
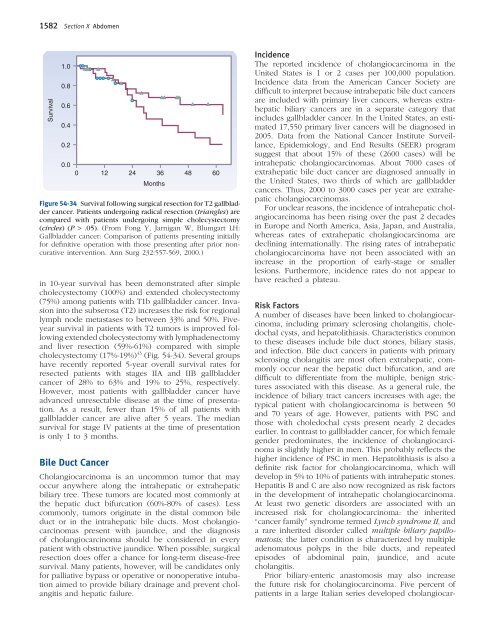
Figure <strong>54</strong>-34 Survival following surgical resection for T2 gallbladder<br />
cancer. Patients undergoing radical resection (triangles) are<br />
compared with patients undergoing simple cholecystectomy<br />
(circles) (P > .05). (From Fong Y, Jarnigan W, Blumgart LH:<br />
Gallbladder cancer: Comparison of patients presenting initially<br />
for defi nitive operation with those presenting after prior noncurative<br />
intervention. Ann Surg 232:557-569, 2000.)<br />
in 10-year survival has been demonstrated after simple<br />
cholecystectomy (100%) and extended cholecystectomy<br />
(75%) among patients with T1b gallbladder cancer. Invasion<br />
into the subserosa (T2) increases the risk for regional<br />
lymph node metastases to between 33% and 50%. Fiveyear<br />
survival in patients with T2 tumors is improved following<br />
extended cholecystectomy with lymphadenectomy<br />
and liver resection (59%-61%) compared with simple<br />
cholecystectomy (17%-19%) 43 (Fig. <strong>54</strong>-34). Several groups<br />
have recently reported 5-year overall survival rates for<br />
resected patients with stages IIA and IIB gallbladder<br />
cancer of 28% to 63% and 19% to 25%, respectively.<br />
However, most patients with gallbladder cancer have<br />
advanced unresectable disease at the time of presentation.<br />
As a result, fewer than 15% of all patients with<br />
gallbladder cancer are alive after 5 years. The median<br />
survival for stage IV patients at the time of presentation<br />
is only 1 to 3 months.<br />
Bile Duct Cancer<br />
<strong>Ch</strong>olangiocarcinoma is an uncommon tumor that may<br />
occur anywhere along the intrahepatic or extrahepatic<br />
biliary tree. These tumors are located most commonly at<br />
the hepatic duct bifurcation (60%-80% of cases). Less<br />
commonly, tumors originate in the distal common bile<br />
duct or in the intrahepatic bile ducts. Most cholangiocarcinomas<br />
present with jaundice, and the diagnosis<br />
of cholangiocarcinoma should be considered in every<br />
patient with obstructive jaundice. When possible, surgical<br />
resection does offer a chance for long-term disease-free<br />
survival. Many patients, however, will be candidates only<br />
for palliative bypass or operative or nonoperative intubation<br />
aimed to provide biliary drainage and prevent cholangitis<br />
and hepatic failure.<br />
Incidence<br />
The reported incidence of cholangiocarcinoma in the<br />
United States is 1 or 2 cases per 100,000 population.<br />
Incidence data from the American Cancer Society are<br />
diffi cult to interpret because intrahepatic bile duct cancers<br />
are included with primary liver cancers, whereas extrahepatic<br />
biliary cancers are in a separate category that<br />
includes gallbladder cancer. In the United States, an estimated<br />
17,550 primary liver cancers will be diagnosed in<br />
2005. Data from the National Cancer Institute Surveillance,<br />
Epidemiology, and End Results (SEER) program<br />
suggest that about 15% of these (2600 cases) will be<br />
intrahepatic cholangiocarcinomas. About 7000 cases of<br />
extrahepatic bile duct cancer are diagnosed annually in<br />
the United States, two thirds of which are gallbladder<br />
cancers. Thus, 2000 to 3000 cases per year are extrahepatic<br />
cholangiocarcinomas.<br />
For unclear reasons, the incidence of intrahepatic cholangiocarcinoma<br />
has been rising over the past 2 decades<br />
in Europe and North America, Asia, Japan, and Australia,<br />
whereas rates of extrahepatic cholangiocarcinoma are<br />
declining internationally. The rising rates of intrahepatic<br />
cholangiocarcinoma have not been associated with an<br />
increase in the proportion of early-stage or smaller<br />
lesions. Furthermore, incidence rates do not appear to<br />
have reached a plateau.<br />
Risk Factors<br />
A number of diseases have been linked to cholangiocarcinoma,<br />
including primary sclerosing cholangitis, choledochal<br />
cysts, and hepatolithiasis. <strong>Ch</strong>aracteristics common<br />
to these diseases include bile duct stones, biliary stasis,<br />
and infection. Bile duct cancers in patients with primary<br />
sclerosing cholangitis are most often extrahepatic, commonly<br />
occur near the hepatic duct bifurcation, and are<br />
diffi cult to differentiate from the multiple, benign strictures<br />
associated with this disease. As a general rule, the<br />
incidence of biliary tract cancers increases with age; the<br />
typical patient with cholangiocarcinoma is between 50<br />
and 70 years of age. However, patients with PSC and<br />
those with choledochal cysts present nearly 2 decades<br />
earlier. In contrast to gallbladder cancer, for which female<br />
gender predominates, the incidence of cholangiocarcinoma<br />
is slightly higher in men. This probably refl ects the<br />
higher incidence of PSC in men. Hepatolithiasis is also a<br />
defi nite risk factor for cholangiocarcinoma, which will<br />
develop in 5% to 10% of patients with intrahepatic stones.<br />
Hepatitis B and C are also now recognized as risk factors<br />
in the development of intrahepatic cholangiocarcinoma.<br />
At least two genetic disorders are associated with an<br />
increased risk for cholangiocarcinoma: the inherited<br />
“cancer family” syndrome termed Lynch syndrome II, and<br />
a rare inherited disorder called multiple biliary papillomatosis;<br />
the latter condition is characterized by multiple<br />
adenomatous polyps in the bile ducts, and repeated<br />
episodes of abdominal pain, jaundice, and acute<br />
cholangitis.<br />
Prior biliary-enteric anastomosis may also increase<br />
the future risk for cholangiocarcinoma. Five percent of<br />
patients in a large Italian series developed cholangiocar-