Ch. 54 – Biliary System
Ch. 54 – Biliary System
Ch. 54 – Biliary System

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
15<strong>54</strong> Section X Abdomen<br />
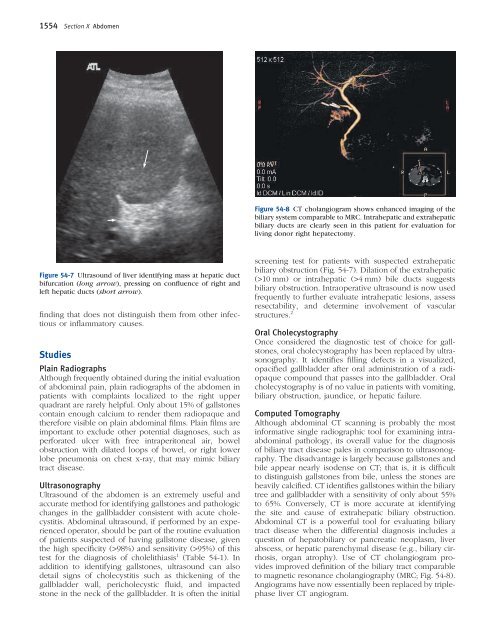
Figure <strong>54</strong>-7 Ultrasound of liver identifying mass at hepatic duct<br />
bifurcation (long arrow), pressing on confl uence of right and<br />
left hepatic ducts (short arrow).<br />
fi nding that does not distinguish them from other infectious<br />
or infl ammatory causes.<br />
Studies<br />
Plain Radiographs<br />
Although frequently obtained during the initial evaluation<br />
of abdominal pain, plain radiographs of the abdomen in<br />
patients with complaints localized to the right upper<br />
quadrant are rarely helpful. Only about 15% of gallstones<br />
contain enough calcium to render them radiopaque and<br />
therefore visible on plain abdominal fi lms. Plain fi lms are<br />
important to exclude other potential diagnoses, such as<br />
perforated ulcer with free intraperitoneal air, bowel<br />
obstruction with dilated loops of bowel, or right lower<br />
lobe pneumonia on chest x-ray, that may mimic biliary<br />
tract disease.<br />
Ultrasonography<br />
Ultrasound of the abdomen is an extremely useful and<br />
accurate method for identifying gallstones and pathologic<br />
changes in the gallbladder consistent with acute cholecystitis.<br />
Abdominal ultrasound, if performed by an experienced<br />
operator, should be part of the routine evaluation<br />
of patients suspected of having gallstone disease, given<br />
the high specifi city (>98%) and sensitivity (>95%) of this<br />
test for the diagnosis of cholelithiasis 1 (Table <strong>54</strong>-1). In<br />
addition to identifying gallstones, ultrasound can also<br />
detail signs of cholecystitis such as thickening of the<br />
gallbladder wall, pericholecystic fl uid, and impacted<br />
stone in the neck of the gallbladder. It is often the initial<br />
Figure <strong>54</strong>-8 CT cholangiogram shows enhanced imaging of the<br />
biliary system comparable to MRC. Intrahepatic and extrahepatic<br />
biliary ducts are clearly seen in this patient for evaluation for<br />
living donor right hepatectomy.<br />
screening test for patients with suspected extrahepatic<br />
biliary obstruction (Fig. <strong>54</strong>-7). Dilation of the extrahepatic<br />
(>10 mm) or intrahepatic (>4 mm) bile ducts suggests<br />
biliary obstruction. Intraoperative ultrasound is now used<br />
frequently to further evaluate intrahepatic lesions, assess<br />
resectability, and determine involvement of vascular<br />
structures. 2<br />
Oral <strong>Ch</strong>olecystography<br />
Once considered the diagnostic test of choice for gallstones,<br />
oral cholecystography has been replaced by ultrasonography.<br />
It identifi es fi lling defects in a visualized,<br />
opacifi ed gallbladder after oral administration of a radiopaque<br />
compound that passes into the gallbladder. Oral<br />
cholecystography is of no value in patients with vomiting,<br />
biliary obstruction, jaundice, or hepatic failure.<br />
Computed Tomography<br />
Although abdominal CT scanning is probably the most<br />
informative single radiographic tool for examining intraabdominal<br />
pathology, its overall value for the diagnosis<br />
of biliary tract disease pales in comparison to ultrasonography.<br />
The disadvantage is largely because gallstones and<br />
bile appear nearly isodense on CT; that is, it is diffi cult<br />
to distinguish gallstones from bile, unless the stones are<br />
heavily calcifi ed. CT identifi es gallstones within the biliary<br />
tree and gallbladder with a sensitivity of only about 55%<br />
to 65%. Conversely, CT is more accurate at identifying<br />
the site and cause of extrahepatic biliary obstruction.<br />
Abdominal CT is a powerful tool for evaluating biliary<br />
tract disease when the differential diagnosis includes a<br />
question of hepatobiliary or pancreatic neoplasm, liver<br />
abscess, or hepatic parenchymal disease (e.g., biliary cirrhosis,<br />
organ atrophy). Use of CT cholangiogram provides<br />
improved defi nition of the biliary tract comparable<br />
to magnetic resonance cholangiography (MRC; Fig. <strong>54</strong>-8).<br />
Angiograms have now essentially been replaced by triplephase<br />
liver CT angiogram.