Ch. 54 – Biliary System
Ch. 54 – Biliary System
Ch. 54 – Biliary System

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
1552 Section X Abdomen<br />
Suspect common<br />
bile duct stones<br />
Lap cholecystectomy<br />
with IOC and lap CDBE<br />
or<br />
ERCP with stone extraction,<br />
papillotomy; lap cholecystectomy<br />
sphincter pressure relaxes in coordination with gallbladder<br />
contraction, thereby allowing the passive fl ow of bile<br />
into the duodenum. During fasting, high-pressure phasic<br />
contractions of the sphincter of Oddi persist through all<br />
phases of the MMC. Sphincter of Oddi activity appears<br />
to be coordinated with the partial gallbladder emptying<br />
and increases in the bile fl ow that occur during phase III<br />
of the MMC. This activity may be a preventive mechanism<br />
against the accumulation of biliary crystals during<br />
fasting.<br />
GENERAL CONSIDERATIONS IN BILIARY<br />
TRACT PATHOPHYSIOLOGY<br />
Suspect extrahepatic<br />
biliary obstruction<br />
Ultrasound<br />
Symptoms<br />
Symptoms attributable to biliary tract pathology are<br />
usually the result of obstruction, infection, or both.<br />
Obstruction can be extramural (e.g., pancreatic cancer),<br />
intramural (cholangiocarcinoma), or intraluminal (cho-<br />
Jaundice<br />
History and physical<br />
Dilated ducts Normal ducts<br />
Proximal obstruction<br />
Palliative<br />
PTC<br />
Suspect malignant<br />
obstruction<br />
3-phase<br />
CT scan<br />
with venous delay<br />
Operation<br />
Suspect intrahepatic<br />
disease<br />
CT scan to rule out liver mass<br />
Hepatitis screen<br />
Possible liver biopsy<br />
Distal obstruction<br />
Palliative<br />
ERCP<br />
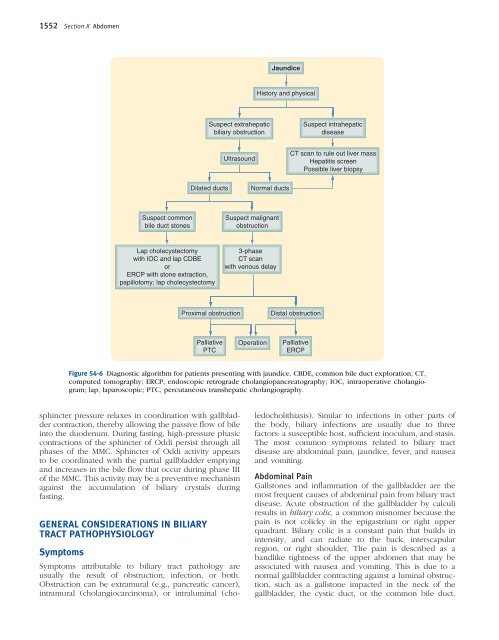
Figure <strong>54</strong>-6 Diagnostic algorithm for patients presenting with jaundice. CBDE, common bile duct exploration; CT,<br />
computed tomography; ERCP, endoscopic retrograde cholangiopancreatography; IOC, intraoperative cholangiogram;<br />
lap, laparoscopic; PTC, percutaneous transhepatic cholangiography.<br />
ledocholithiasis). Similar to infections in other parts of<br />
the body, biliary infections are usually due to three<br />
factors: a susceptible host, suffi cient inoculum, and stasis.<br />
The most common symptoms related to biliary tract<br />
disease are abdominal pain, jaundice, fever, and nausea<br />
and vomiting.<br />
Abdominal Pain<br />
Gallstones and infl ammation of the gallbladder are the<br />
most frequent causes of abdominal pain from biliary tract<br />
disease. Acute obstruction of the gallbladder by calculi<br />
results in biliary colic, a common misnomer because the<br />
pain is not colicky in the epigastrium or right upper<br />
quadrant. <strong>Biliary</strong> colic is a constant pain that builds in<br />
intensity, and can radiate to the back, interscapular<br />
region, or right shoulder. The pain is described as a<br />
bandlike tightness of the upper abdomen that may be<br />
associated with nausea and vomiting. This is due to a<br />
normal gallbladder contracting against a luminal obstruction,<br />
such as a gallstone impacted in the neck of the<br />
gallbladder, the cystic duct, or the common bile duct.