Ch. 54 – Biliary System
Ch. 54 – Biliary System
Ch. 54 – Biliary System

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
is jaundice with or without abdominal pain. Patients<br />
may also present months or years after prior surgery<br />
with cholangitis or cirrhosis secondary to a biliary tract<br />
injury.<br />
Diagnosis and Management<br />
The management of bile duct injury is dependent on the<br />
timing of diagnosis and extent and level of injury. Inappropriate<br />
management of biliary strictures may result in<br />
signifi cant morbidity and mortality secondary to complications<br />
such as biliary cirrhosis or cholangitis. In a 12year<br />
review of 130 patients with postoperative biliary<br />
strictures, the causes of mortality were all related to the<br />
presence of liver parenchymal disease with portal hypertension.<br />
Twenty-three of these patients had evidence of<br />
portal hypertension at the time of referral. 27<br />
Management of the Bile Duct Injury Recognized at the Time<br />
of <strong>Ch</strong>olecystectomy Isolated, small, non<strong>–</strong>cautery-based<br />
partial lateral bile duct injury recognized at time of cholecystectomy<br />
can be managed with placement of a T<br />
tube. The T tube can be placed at the site of the injury<br />
if this is similar in size to a choledochotomy. However,<br />
if the biliary injury is more extensive, or if there is signifi<br />
cant thermal damage owing to cautery-based trauma,<br />
or if the injury involves more than 50% of the circumference<br />
of the bile duct wall, an end-to-side choledochojejunostomy<br />
with a Roux-en-Y loop of jejunum should be<br />
performed. Similarly, major bile duct injuries, including<br />
transections of the common bile or common hepatic<br />
duct, can be repaired if recognized at the time of cholecystectomy.<br />
Isolated hepatic ducts smaller than 3 mm or<br />
those draining a single hepatic segment can be safely<br />
ligated. Ducts larger than 3 mm are more likely to drain<br />
several segments or an entire lobe and need to be reimplanted.<br />
It cannot be overstated that signifi cant experience<br />
and judgment are critical to the decision to conduct<br />
a repair at the time of injury. If one is uncertain or underexperienced,<br />
and no colleague with suffi cient expertise<br />
is immediately available, placing a drain followed by<br />
referral to an experienced center is the most appropriate<br />
course of action.<br />
Management of the Bile Duct Injury Recognized After <strong>Ch</strong>olecystectomy<br />
Most large series report the incidence of ductal<br />
injury after laparoscopic cholecystectomy to be 0.3% to<br />
0.85%. Historically, after open cholecystectomy, 10% of<br />
patients presented within the fi rst week, 70% within 6<br />
months, and 80% within 1 year. In a recent study of 156<br />
patients referred for management of biliary strictures<br />
resulting from bile duct injuries, 9.3% of injuries were<br />
recognized during laparoscopic versus 0% during open<br />
cholecystectomy. 28 In this series of 156 patients with<br />
postoperative biliary strictures, 49 patients (31.4%) presented<br />
with leaks, 42 (26.9%) presented with jaundice,<br />
and 50 (32.1%) presented with cholangitis. 28 In general,<br />
patients with a bile leak will present early, whereas<br />
patients with postoperative biliary strictures alone often<br />
present with jaundice or cholangitis months to years after<br />
the initial injury.<br />
Diagnosis Abdominal imaging with ultrasonography or<br />
CT should be performed in patients with signs of abdominal<br />
pain or peritonitis, sepsis, or any other clinical sus-<br />
<strong>Ch</strong>apter <strong>54</strong> <strong>Biliary</strong> <strong>System</strong> 1569<br />
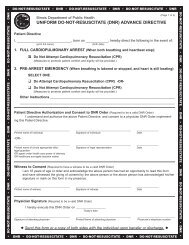
Figure <strong>54</strong>-21 Transhepatic cholangiography confi rming ligation<br />
of the common hepatic duct just distal to the bifurcation<br />
(arrow).<br />
picion of biloma. Such patients must be stabilized with<br />
immediate parenteral antibiotics and image-guided percutaneous<br />
drainage of any fl uid collections. Patients with<br />
signs and symptoms of cholangitis should undergo urgent<br />
cholangiogram with bile duct drainage. <strong>Ch</strong>olangiography<br />
should be performed to establish the presence of ductal<br />
stricture, identify the level of the stricture, and identify<br />
the nature of the injury when necessary. In one study of<br />
88 patients with bile duct injuries from laparoscopic cholecystectomy,<br />
attempts at repair were unsuccessful in 27<br />
of 28 (96%) when preoperative cholangiograms were not<br />
performed, and 69% unsuccessful when data from cholangiograms<br />
were incomplete. 29 It is important that the<br />
method of cholangiography should provide detail of the<br />
intrahepatic ductal system and the bile duct confl uence.<br />
Although PTC is the imaging method of choice for most<br />
postoperative biliary strictures, expertise with this is not<br />
available at all centers (Fig. <strong>54</strong>-21). ERCP may be easier<br />
to obtain in a patient with a biliary stricture and cholangitis<br />
who requires urgent cholangiography and biliary<br />
decompression. However, this is only useful in patients<br />
with bile duct continuity. Cystic duct leaks or small tangential<br />
injuries can be treated with endoscopic stenting.<br />
In situations in which the biliary stricture is too tight to<br />
pass with ERCP, PTC may be performed for proximal<br />
biliary decompression.<br />
CT arteriography should be considered in the preoperative<br />
evaluation of patients with benign biliary