Occupation and cancer - European Trade Union Institute (ETUI)
Occupation and cancer - European Trade Union Institute (ETUI)
Occupation and cancer - European Trade Union Institute (ETUI)

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Acta Oncol Downloaded from informahealthcare.com by 212.35.100.66 on 04/06/11<br />
For personal use only.<br />
time of the census. These differences will probably<br />
not have affected the classification of men, but parttime<br />
working women could have been classified<br />
differently across the countries. There are differences<br />
across the countries in the way a distinction<br />
was made between economically inactive housewives<br />
<strong>and</strong> economically active housewives at the family<br />
farm or in the family shop.<br />
The proportion of economically inactive men of<br />
the total 30 64-year-old male population at the time<br />
of the first available population census of the current<br />
study was 7.3%, including a great proportion of men<br />
unable to work, for instance due to a disease. The<br />
large category of economically inactive women<br />
(42.4% of the total 30 64-year-old female population)<br />
included housewives <strong>and</strong> farmers’ spouses not<br />
taking part in farm work <strong>and</strong> was thus less selected in<br />
terms of health status than that of males.<br />
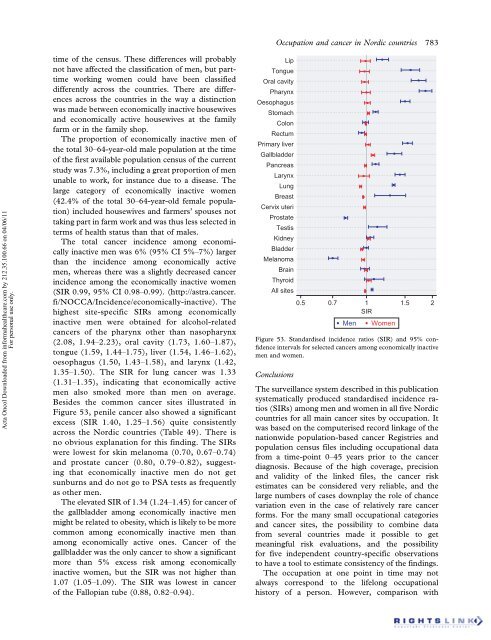
The total <strong>cancer</strong> incidence among economically<br />
inactive men was 6% (95% CI 5% 7%) larger<br />
than the incidence among economically active<br />
men, whereas there was a slightly decreased <strong>cancer</strong><br />
incidence among the economically inactive women<br />
(SIR 0.99, 95% CI 0.98 0.99). (http://astra.<strong>cancer</strong>.<br />
fi/NOCCA/Incidence/economically-inactive). The<br />
highest site-specific SIRs among economically<br />
inactive men were obtained for alcohol-related<br />
<strong>cancer</strong>s of the pharynx other than nasopharynx<br />
(2.08, 1.94 2.23), oral cavity (1.73, 1.60 1.87),<br />
tongue (1.59, 1.44 1.75), liver (1.54, 1.46 1.62),<br />
oesophagus (1.50, 1.43 1.58), <strong>and</strong> larynx (1.42,<br />
1.35 1.50). The SIR for lung <strong>cancer</strong> was 1.33<br />
(1.31 1.35), indicating that economically active<br />
men also smoked more than men on average.<br />
Besides the common <strong>cancer</strong> sites illustrated in<br />
Figure 53, penile <strong>cancer</strong> also showed a significant<br />
excess (SIR 1.40, 1.25 1.56) quite consistently<br />
across the Nordic countries (Table 49). There is<br />
no obvious explanation for this finding. The SIRs<br />
were lowest for skin melanoma (0.70, 0.67 0.74)<br />
<strong>and</strong> prostate <strong>cancer</strong> (0.80, 0.79 0.82), suggesting<br />
that economically inactive men do not get<br />
sunburns <strong>and</strong> do not go to PSA tests as frequently<br />
as other men.<br />
The elevated SIR of 1.34 (1.24 1.45) for <strong>cancer</strong> of<br />
the gallbladder among economically inactive men<br />
might be related to obesity, which is likely to be more<br />
common among economically inactive men than<br />
among economically active ones. Cancer of the<br />
gallbladder was the only <strong>cancer</strong> to show a significant<br />
more than 5% excess risk among economically<br />
inactive women, but the SIR was not higher than<br />
1.07 (1.05 1.09). The SIR was lowest in <strong>cancer</strong><br />
of the Fallopian tube (0.88, 0.82 0.94).<br />
Lip<br />
Tongue<br />
Oral cavity<br />
Pharynx<br />
Oesophagus<br />
Stomach<br />
Colon<br />
Rectum<br />
Primary liver<br />
Gallbladder<br />
Pancreas<br />
Larynx<br />
Lung<br />
Breast<br />
Cervix uteri<br />
Prostate<br />
Testis<br />
Kidney<br />
Bladder<br />
Melanoma<br />
Brain<br />
Thyroid<br />
All sites<br />
<strong>Occupation</strong> <strong>and</strong> <strong>cancer</strong> in Nordic countries 783<br />
0.5 0.7 1<br />
SIR<br />
1.5 2<br />
Men Women<br />
Figure 53. St<strong>and</strong>ardised incidence ratios (SIR) <strong>and</strong> 95% confidence<br />
intervals for selected <strong>cancer</strong>s among economically inactive<br />
men <strong>and</strong> women.<br />
Conclusions<br />
The surveillance system described in this publication<br />
systematically produced st<strong>and</strong>ardised incidence ratios<br />
(SIRs) among men <strong>and</strong> women in all five Nordic<br />
countries for all main <strong>cancer</strong> sites by occupation. It<br />
was based on the computerised record linkage of the<br />
nationwide population-based <strong>cancer</strong> Registries <strong>and</strong><br />
population census files including occupational data<br />
from a time-point 0 45 years prior to the <strong>cancer</strong><br />
diagnosis. Because of the high coverage, precision<br />
<strong>and</strong> validity of the linked files, the <strong>cancer</strong> risk<br />
estimates can be considered very reliable, <strong>and</strong> the<br />
large numbers of cases downplay the role of chance<br />
variation even in the case of relatively rare <strong>cancer</strong><br />
forms. For the many small occupational categories<br />
<strong>and</strong> <strong>cancer</strong> sites, the possibility to combine data<br />
from several countries made it possible to get<br />
meaningful risk evaluations, <strong>and</strong> the possibility<br />
for five independent country-specific observations<br />
to have a tool to estimate consistency of the findings.<br />
The occupation at one point in time may not<br />
always correspond to the lifelong occupational<br />
history of a person. However, comparison with