Full Report
Full Report
Full Report

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
INTRODUCTION<br />
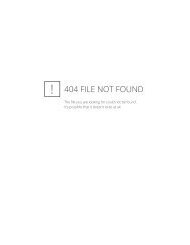
FIGURE 2<br />
Expanded Chronic Care Model<br />
COMMUNITY<br />
Build Healthy<br />
Public Policy<br />
Create<br />
supportive<br />
environments<br />
Strenghten<br />
community<br />
action<br />
Health System<br />
Self-management/<br />
develop<br />
personal skills<br />
Delivery System<br />
Design/Re-orient<br />
health services<br />
Decision<br />
support<br />
Information<br />
systems<br />
ACTIVATED<br />
COMMUNITY<br />
Informed<br />
activated<br />
patient<br />
PRODUCTIVE<br />
Interactions &<br />
Relationships<br />
Prepared, proactive<br />
practice team<br />
PREPARED,<br />
PROACTIVE<br />
COMMUNITY<br />
(PARTNERS)<br />
Working from both the prevention and treatment ends of the care continuum – and engaging community support as well as healthcare<br />
expertise – offers the best potential for improved long-term health outcomes.<br />
Each improvement team brought together<br />
healthcare executives, policy-makers and<br />
clinical leaders to assess, design and support<br />
project implementation.<br />
A strong evidence base<br />
The Expanded Chronic Care Model (ECCM; Figure 2)<br />
provided the guiding frame for the CDM project. The<br />
ECCM shows how population health promotion and<br />
clinical health services can complement one another<br />
to improve the health of, and healthcare provided to,<br />
patients and communities. 1 The Department decided<br />
to focus on four ECCM elements that are essential in<br />
the management of chronic disease:<br />
• Self management – Recognize patients as experts<br />
in their own care and develop their skills and<br />
confidence to manage their condition through<br />
education, coaching and linking to resources.<br />
• Health system design – Coordinate care,<br />
use practitioners to their full scope of practice,<br />
and improve access to care.<br />
• Decision support – Establish evidence-based<br />
guidelines to ensure that quality care is consistently<br />
delivered by all healthcare providers.<br />
• Information systems – Effectively gather,<br />
share and use information and data.<br />
The Department used tracer methodology * to examine<br />
each of these elements strictly in the context of the<br />
targeted conditions: diabetes, renal disease, and mental<br />
health. In tracer methodology, patients are followed<br />
through the continuum of care, and the systems of care<br />
are reviewed. The process helps uncover problematic<br />
practices, policies and other intrinsic issues that result in<br />
fragmented care – many of which are common among<br />
various chronic diseases.<br />
*<br />
Kessner tracer methodology (1973)<br />
9<br />
Making the Case for Change