

Antimicrobial Use Guidelines (AMUG) version 21 - UW Health
Antimicrobial Use Guidelines (AMUG) version 21 - UW Health
Antimicrobial Use Guidelines (AMUG) version 21 - UW Health

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
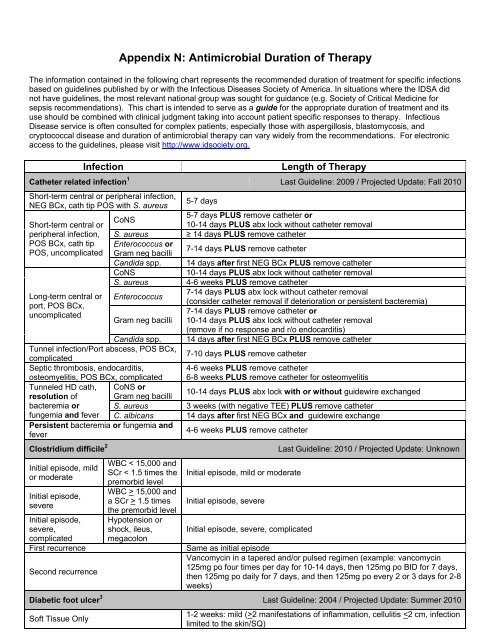
Appendix N: <strong>Antimicrobial</strong> Duration of TherapyThe information contained in the following chart represents the recommended duration of treatment for specific infectionsbased on guidelines published by or with the Infectious Diseases Society of America. In situations where the IDSA didnot have guidelines, the most relevant national group was sought for guidance (e.g. Society of Critical Medicine forsepsis recommendations). This chart is intended to serve as a guide for the appropriate duration of treatment and itsuse should be combined with clinical judgment taking into account patient specific responses to therapy. InfectiousDisease service is often consulted for complex patients, especially those with aspergillosis, blastomycosis, andcryptococcal disease and duration of antimicrobial therapy can vary widely from the recommendations. For electronicaccess to the guidelines, please visit http://www.idsociety.org.InfectionLength of TherapyCatheter related infection 1 Last Guideline: 2009 / Projected Update: Fall 2010Short-term central or peripheral infection,NEG BCx, cath tip POS with S. aureusShort-term central orperipheral infection,POS BCx, cath tipPOS, uncomplicatedLong-term central orport, POS BCx,uncomplicatedCoNS5-7 days5-7 days PLUS remove catheter or10-14 days PLUS abx lock without catheter removalS. aureus ≥ 14 days PLUS remove catheterEnterococcus orGram neg bacilli7-14 days PLUS remove catheterCandida spp. 14 days after first NEG BCx PLUS remove catheterCoNS10-14 days PLUS abx lock without catheter removalS. aureus 4-6 weeks PLUS remove catheterEnterococcus7-14 days PLUS abx lock without catheter removal(consider catheter removal if deterioration or persistent bacteremia)7-14 days PLUS remove catheter orGram neg bacilli 10-14 days PLUS abx lock without catheter removal(remove if no response and r/o endocarditis)Candida spp. 14 days after first NEG BCx PLUS remove catheterTunnel infection/Port abscess, POS BCx,complicated7-10 days PLUS remove catheterSeptic thrombosis, endocarditis,osteomyelitis, POS BCx, complicated4-6 weeks PLUS remove catheter6-8 weeks PLUS remove catheter for osteomyelitisTunneled HD cath, CoNS orresolution of Gram neg bacilli10-14 days PLUS abx lock with or without guidewire exchangedbacteremia or S. aureus 3 weeks (with negative TEE) PLUS remove catheterfungemia and fever C. albicans 14 days after first NEG BCx and guidewire exchangePersistent bacteremia or fungemia andfever4-6 weeks PLUS remove catheterClostridium difficile 2Initial episode, mildor moderateInitial episode,severeInitial episode,severe,complicatedFirst recurrenceSecond recurrenceWBC < 15,000 andSCr < 1.5 times thepremorbid levelWBC > 15,000 anda SCr > 1.5 timesthe premorbid levelHypotension orshock, ileus,megacolonInitial episode, mild or moderateInitial episode, severeInitial episode, severe, complicatedLast Guideline: 2010 / Projected Update: UnknownSame as initial episodeVancomycin in a tapered and/or pulsed regimen (example: vancomycin125mg po four times per day for 10-14 days, then 125mg po BID for 7 days,then 125mg po daily for 7 days, and then 125mg po every 2 or 3 days for 2-8weeks)Diabetic foot ulcer 3 Last Guideline: 2004 / Projected Update: Summer 2010Soft Tissue Only1-2 weeks: mild (>2 manifestations of inflammation, cellulitis













