44Hanna Styczyńska et al.INTRODUCTIONThe attainment of peak bone mass in women typicallytakes place in the early 30s but pregnancy <strong>and</strong>lactation occur mostly during or before this period oflife. It is considered that pregnancy could affect peakbone mass <strong>and</strong> increase the risk of developing osteoporosislater in life [1]. Bone loss during pregnancy mayresult in pregnancy-associated osteoporosis <strong>and</strong> vertebralfractures [2, 3].During pregnancy, about 30 g of calcium is transferredto a full term neonate [4]. Approximately 80%of calcium accumulates during the third trimester,when the fetal skeleton is rapidly mineralizing. Althoughmaternal adaptations designed to meet the calciumneeds of the fetus might begin early in pregnancy,they are most needed in the third trimester [5-6]. Calcium homeostasis appears to be attained byincreased dietary intake with or without increasedefficiency of absorption, decreased urinary excretion asa result of increased tubular calcium resorption <strong>and</strong> byelevated bone turnover with bone loss [7].Several studies showed a decrease in BMD duringpregnancy even up to 5%. Thus, there seems to be agood evidence that during pregnancy calcium is mobilizedfrom the maternal skeleton to that of developingfetus. Development of biochemical markers enabled toasses bone turnover during normal pregnancy, whenradiography or densitometry cannot be used [8-10].The mechanisms regulating bone turnover duringpregnancy are not well known [11]. RANK - a cellularreceptor activator of NF-kappaB, RANK-lig<strong>and</strong> <strong>and</strong>osteoprotegerin (OPG) constitute a novel cytokinesystem that regulate activity of bone cells. Osteoprotegerin,is a soluble decoy receptor that inhibits boneresorption by binding to receptor activator of nuclearfactor NF-kappaB lig<strong>and</strong> (RANKL) <strong>and</strong> in consequenceinhibits osteoclast’s maturation <strong>and</strong> activation[12]. RANKL produced by osteoblastic lineage cells<strong>and</strong> activated T lymphocytes is the essential factor forosteoclastogenesis, fusion, activation <strong>and</strong> survival ofosteoclasts, thus effecting on bone resorption <strong>and</strong> boneloss. RANKL activates its specific receptor-RANK,located on osteoclasts <strong>and</strong> its signalling cascade involvesstimulation of osteoclasts action. The effects ofRANKL are counteracted by OPG which acts asa soluble neutralizing receptor.RANKL <strong>and</strong> OPG are regulated by various hormones(glucocorticoids, vitamin D, estrogens), cytokines(tumour necrosis factor alpha, interleukins1,4,6,11 <strong>and</strong> 17) <strong>and</strong> various mesenchymal transcriptionfactors. RANKL <strong>and</strong> OPG are also importantregulators of vascular biology <strong>and</strong> calcification <strong>and</strong> ofthe development of a lactating mammary gl<strong>and</strong> duringpregnancy. OPG was also found in placenta [13]. Allthis indicates a crucial role for this system in extraskeletalcalcium h<strong>and</strong>ling [14]. The discovery <strong>and</strong> characterizationof RANKL, RANK, OPG <strong>and</strong> subsequentstudies have changed the concept of bone <strong>and</strong> calciummetabolism.The objective of the study was to assess bone turnoverin pregnancy by measuring biochemical bonemarkers in the serum in relation to osteoprotegerinlevel.PARTICIPANTS AND SAMPLE COLLECTIONThirty healthy, pregnant women during their firstvisit for prenatal care participated in our study. Exclusioncriteria included assisted conception or any diseasesor use of medication known to affect bone metabolism.All pregnant women were primiparas ofmean age 24.5±3.8 yrs (20-36 yrs) <strong>and</strong> body massindex (BMI) before pregnancy 20.3±2.8 kg/m2 (16.7-30.9). Most of women fulfilled 50-75% of recommendeddaily calcium requirement.27 healthy, non pregnant women, before first pregnancy,(mean age, 25±3.4 yrs; range 21-33 yrs, meanBMI 20.9±2.9 ; range 17.6-29.8) served as controls.The average calcium intake in most of non-pregnantwomen was on the level of 50-75% of daily requirement.The study protocol was approved by the local BioethicalCommittee of <strong>Collegium</strong> <strong>Medicum</strong>, N.C. Universityin Bydgoszcz. All participants gave theirinformed written consent.MATERIALS AND METHODSFasting blood samples from pregnant women werecollected, between 8-9 am, at 1 st trimester (6-14 wks)<strong>and</strong> at 3 rd trimester (31-37 wks) of pregnancy. In controlgroup fasting blood samples were taken once inautumn/winter season. Serum was immediately sepa-
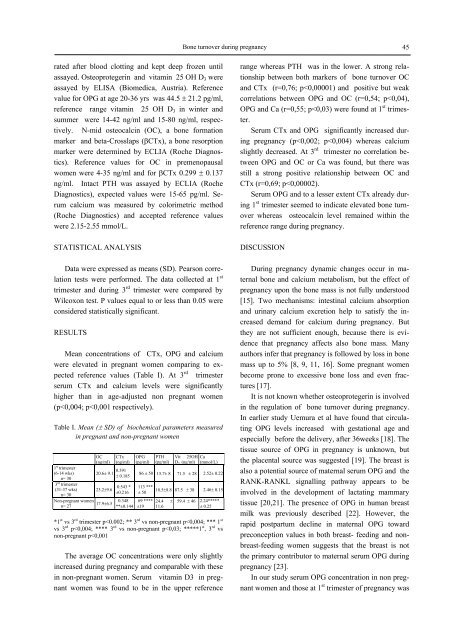
Bone turnover during pregnancy 45rated after blood clotting <strong>and</strong> kept deep frozen untilassayed. Osteoprotegerin <strong>and</strong> vitamin 25 OH D 3 wereassayed by ELISA (Biomedica, Austria). Referencevalue for OPG at age 20-36 yrs was 44.5 ± 21.2 pg/ml,reference range vitamin 25 OH D 3 in winter <strong>and</strong>summer were 14-42 ng/ml <strong>and</strong> 15-80 ng/ml, respectively.N-mid osteocalcin (OC), a bone formationmarker <strong>and</strong> beta-Crosslaps (βCTx), a bone resorptionmarker were determined by ECLIA (Roche Diagnostics).Reference values for OC in premenopausalwomen were 4-35 ng/ml <strong>and</strong> for βCTx 0.299 ± 0.137ng/ml. Intact PTH was assayed by ECLIA (RocheDiagnostics), expected values were 15-65 pg/ml. Serumcalcium was measured by colorimetric method(Roche Diagnostics) <strong>and</strong> accepted reference valueswere 2.15-2.55 mmol/L.STATISTICAL ANALYSISData were expressed as means (SD). Pearson correlationtests were performed. The data collected at 1 sttrimester <strong>and</strong> during 3 rd trimester were compared byWilcoxon test. P values equal to or less than 0.05 wereconsidered statistically significant.RESULTSMean concentrations of CTx, OPG <strong>and</strong> calciumwere elevated in pregnant women comparing to expectedreference values (Table I). At 3 rd trimesterserum CTx <strong>and</strong> calcium levels were significantlyhigher than in age-adjusted non pregnant women(p
- Page 8: 8Wojciech J. Baranowskirating) move
- Page 13 and 14: The benefits resulting from introdu
- Page 15 and 16: The benefits resulting from introdu
- Page 17 and 18: Medical and Biological Sciences, 20
- Page 19 and 20: The history and the present of hern
- Page 21 and 22: The history and the present of hern
- Page 23: The history and the present of hern
- Page 26: 26Anna Budzyńska et al.Gram-dodatn
- Page 32 and 33: 32Piotr Kamiński et al.Streszczeni
- Page 34 and 35: 34Piotr Kamiński et al.both in Pom
- Page 36 and 37: 36Piotr Kamiński et al.hemoglobin
- Page 39 and 40: Medical and Biological Sciences, 20
- Page 41 and 42: Impact of mandatory vaccination pro
- Page 43: Medical and Biological Sciences, 20
- Page 47: Bone turnover during pregnancy 47pl
- Page 50 and 51: 50Jan Styczyński, Anna Jaworska(p
- Page 52 and 53: 52Jan Styczyński, Anna JaworskaRES
- Page 55 and 56: Medical and Biological Sciences, 20
- Page 57 and 58: Analysis of immunophenotype at seco
- Page 59: Analysis of immunophenotype at seco
- Page 62 and 63: 62Ana-Maria ŠimundićINTRODUCTIOND
- Page 64 and 65: 64Ana-Maria ŠimundićThe shape of
- Page 67 and 68: Medical and Biological Sciences, 20
- Page 69 and 70: Quantitative anatomy of the aortic
- Page 71 and 72: Quantitative anatomy of the aortic
- Page 73 and 74: Medical and Biological Sciences, 20
- Page 75 and 76: Volumetric growth of various aortic
- Page 77 and 78: Volumetric growth of various aortic
- Page 79 and 80: Medical and Biological Sciences, 20
- Page 81 and 82: Effect of Low Level Laser Therapy a
- Page 83 and 84: Effect of Low Level Laser Therapy a
- Page 85 and 86: Medical and Biological Sciences, 20
- Page 87 and 88: Body weight support during treadmil
- Page 89 and 90: Body weight support during treadmil
- Page 91 and 92: Medical and Biological Sciences, 20