

Adult Medical Emergency Handbook - Scottish Intensive Care Society
Adult Medical Emergency Handbook - Scottish Intensive Care Society
Adult Medical Emergency Handbook - Scottish Intensive Care Society

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
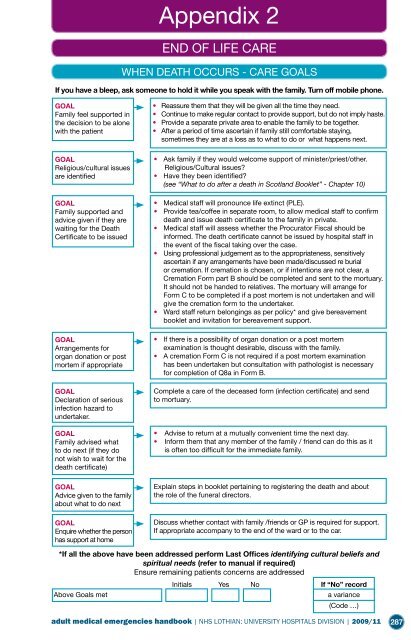
END OF LIFE CARE<br />
WHEN DEATH OCCURS - CARE GOALS<br />
If you have a bleep, ask someone to hold it while you speak with the family. Turn off mobile phone.<br />
GOAL<br />
Family feel supported in<br />
the decision to be alone<br />
with the patient<br />
GOAL<br />
Religious/cultural issues<br />
are identified<br />
GOAL<br />
Family supported and<br />
advice given if they are<br />
waiting for the Death<br />
Certificate to be issued<br />
GOAL<br />
Arrangements for<br />
organ donation or post<br />
mortem if appropriate<br />
GOAL<br />
Declaration of serious<br />
infection hazard to<br />
undertaker.<br />
GOAL<br />
Family advised what<br />
to do next (if they do<br />
not wish to wait for the<br />
death certificate)<br />
GOAL<br />
Advice given to the family<br />
about what to do next<br />
GOAL<br />
Enquire whether the person<br />
has support at home<br />
Appendix 2<br />
• Reassure them that they will be given all the time they need.<br />
• Continue to make regular contact to provide support, but do not imply haste.<br />
• Provide a separate private area to enable the family to be together.<br />
• After a period of time ascertain if family still comfortable staying,<br />
sometimes they are at a loss as to what to do or what happens next.<br />
• Ask family if they would welcome support of minister/priest/other.<br />
Religious/Cultural issues?<br />
• Have they been identified?<br />
(see “What to do after a death in Scotland Booklet” - Chapter 10)<br />
• <strong>Medical</strong> staff will pronounce life extinct (PLE).<br />
• Provide tea/coffee in separate room, to allow medical staff to confirm<br />
death and issue death certificate to the family in private.<br />
• <strong>Medical</strong> staff will assess whether the Procurator Fiscal should be<br />
informed. The death certificate cannot be issued by hospital staff in<br />
the event of the fiscal taking over the case.<br />
• Using professional judgement as to the appropriateness, sensitively<br />
ascertain if any arrangements have been made/discussed re burial<br />
or cremation. If cremation is chosen, or if intentions are not clear, a<br />
Cremation Form part B should be completed and sent to the mortuary.<br />
It should not be handed to relatives. The mortuary will arrange for<br />
Form C to be completed if a post mortem is not undertaken and will<br />
give the cremation form to the undertaker.<br />
• Ward staff return belongings as per policy* and give bereavement<br />
booklet and invitation for bereavement support.<br />
• If there is a possibility of organ donation or a post mortem<br />
examination is thought desirable, discuss with the family.<br />
• A cremation Form C is not required if a post mortem examination<br />
has been undertaken but consultation with pathologist is necessary<br />
for completion of Q8a in Form B.<br />
Complete a care of the deceased form (infection certificate) and send<br />
to mortuary.<br />
• Advise to return at a mutually convenient time the next day.<br />
• Inform them that any member of the family / friend can do this as it<br />
is often too difficult for the immediate family.<br />
Explain steps in booklet pertaining to registering the death and about<br />
the role of the funeral directors.<br />
Discuss whether contact with family /friends or GP is required for support.<br />
If appropriate accompany to the end of the ward or to the car.<br />
*If all the above have been addressed perform Last Offices identifying cultural beliefs and<br />
spiritual needs (refer to manual if required)<br />
Ensure remaining patients concerns are addressed<br />
Initials Yes No If “No” record<br />
Above Goals met a variance<br />
(Code …)<br />
adult medical emergencies handbook | NHS LOTHIAN: UNIVERSITY HOSPITALS DIVISION | 2009/11<br />
287