

Clinical Pharmacology and Therapeutics
A Textbook of Clinical Pharmacology and ... - clinicalevidence
A Textbook of Clinical Pharmacology and ... - clinicalevidence
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
DRUGS USED FOR MIGRAINE PROPHYLAXIS 143<br />
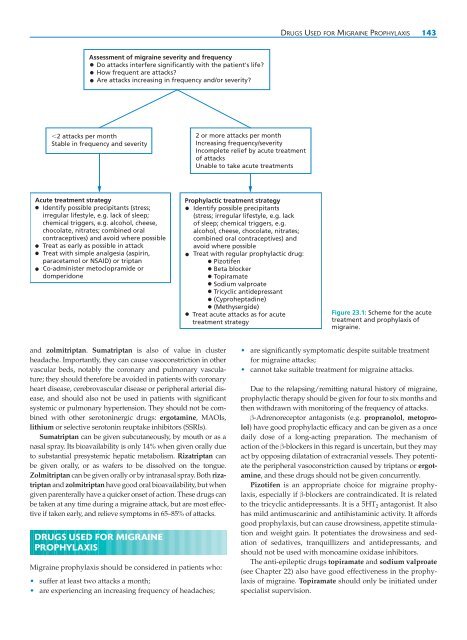
Assessment of migraine severity <strong>and</strong> frequency<br />
Do attacks interfere significantly with the patient's life?<br />
How frequent are attacks?<br />
Are attacks increasing in frequency <strong>and</strong>/or severity?<br />
2 attacks per month<br />
Stable in frequency <strong>and</strong> severity<br />
2 or more attacks per month<br />
Increasing frequency/severity<br />
Incomplete relief by acute treatment<br />
of attacks<br />
Unable to take acute treatments<br />
Acute treatment strategy<br />
Identify possible precipitants (stress;<br />
irregular lifestyle, e.g. lack of sleep;<br />
chemical triggers, e.g. alcohol, cheese,<br />
chocolate, nitrates; combined oral<br />
contraceptives) <strong>and</strong> avoid where possible<br />
Treat as early as possible in attack<br />
Treat with simple analgesia (aspirin,<br />
paracetamol or NSAID) or triptan<br />
Co-administer metoclopramide or<br />
domperidone<br />
Prophylactic treatment strategy<br />
Identify possible precipitants<br />
(stress; irregular lifestyle, e.g. lack<br />
of sleep; chemical triggers, e.g.<br />
alcohol, cheese, chocolate, nitrates;<br />
combined oral contraceptives) <strong>and</strong><br />
avoid where possible<br />
Treat with regular prophylactic drug:<br />
Pizotifen<br />
Beta blocker<br />
Topiramate<br />
Sodium valproate<br />
Tricyclic antidepressant<br />
(Cyproheptadine)<br />
(Methysergide)<br />
Treat acute attacks as for acute<br />
treatment strategy<br />
Figure 23.1: Scheme for the acute<br />
treatment <strong>and</strong> prophylaxis of<br />
migraine.<br />
<strong>and</strong> zolmitriptan. Sumatriptan is also of value in cluster<br />
headache. Importantly, they can cause vasoconstriction in other<br />
vascular beds, notably the coronary <strong>and</strong> pulmonary vasculature;<br />
they should therefore be avoided in patients with coronary<br />
heart disease, cerebrovascular disease or peripheral arterial disease,<br />
<strong>and</strong> should also not be used in patients with significant<br />
systemic or pulmonary hypertension. They should not be combined<br />
with other serotoninergic drugs: ergotamine, MAOIs,<br />
lithium or selective serotonin reuptake inhibitors (SSRIs).<br />
Sumatriptan can be given subcutaneously, by mouth or as a<br />
nasal spray. Its bioavailability is only 14% when given orally due<br />
to substantial presystemic hepatic metabolism. Rizatriptan can<br />
be given orally, or as wafers to be dissolved on the tongue.<br />
Zolmitriptan can be given orally or by intranasal spray. Both rizatriptan<br />
<strong>and</strong> zolmitriptan have good oral bioavailability, but when<br />
given parenterally have a quicker onset of action. These drugs can<br />
be taken at any time during a migraine attack, but are most effective<br />
if taken early, <strong>and</strong> relieve symptoms in 65–85% of attacks.<br />
DRUGS USED FOR MIGRAINE<br />
PROPHYLAXIS<br />
Migraine prophylaxis should be considered in patients who:<br />
• suffer at least two attacks a month;<br />
• are experiencing an increasing frequency of headaches;<br />
• are significantly symptomatic despite suitable treatment<br />
for migraine attacks;<br />
• cannot take suitable treatment for migraine attacks.<br />
Due to the relapsing/remitting natural history of migraine,<br />
prophylactic therapy should be given for four to six months <strong>and</strong><br />
then withdrawn with monitoring of the frequency of attacks.<br />
β-Adrenoreceptor antagonists (e.g. propranolol, metoprolol)<br />
have good prophylactic efficacy <strong>and</strong> can be given as a once<br />
daily dose of a long-acting preparation. The mechanism of<br />
action of the β-blockers in this regard is uncertain, but they may<br />
act by opposing dilatation of extracranial vessels. They potentiate<br />
the peripheral vasoconstriction caused by triptans or ergotamine,<br />
<strong>and</strong> these drugs should not be given concurrently.<br />
Pizotifen is an appropriate choice for migraine prophylaxis,<br />
especially if β-blockers are contraindicated. It is related<br />
to the tricyclic antidepressants. It is a 5HT 2 antagonist. It also<br />
has mild antimuscarinic <strong>and</strong> antihistaminic activity. It affords<br />
good prophylaxis, but can cause drowsiness, appetite stimulation<br />
<strong>and</strong> weight gain. It potentiates the drowsiness <strong>and</strong> sedation<br />
of sedatives, tranquillizers <strong>and</strong> antidepressants, <strong>and</strong><br />
should not be used with monoamine oxidase inhibitors.<br />
The anti-epileptic drugs topiramate <strong>and</strong> sodium valproate<br />
(see Chapter 22) also have good effectiveness in the prophylaxis<br />
of migraine. Topiramate should only be initiated under<br />
specialist supervision.

