

Clinical Pharmacology and Therapeutics
A Textbook of Clinical Pharmacology and ... - clinicalevidence
A Textbook of Clinical Pharmacology and ... - clinicalevidence
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
ANTI-HIV DRUGS 353<br />
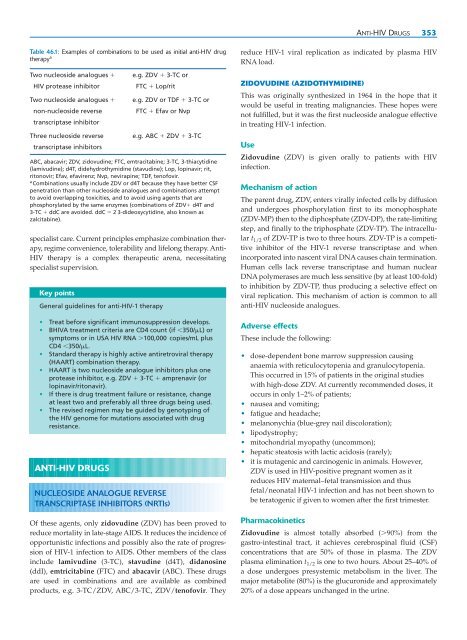
Table 46.1: Examples of combinations to be used as initial anti-HIV drug<br />
therapy a<br />
Two nucleoside analogues <br />
HIV protease inhibitor<br />
Two nucleoside analogues <br />
non-nucleoside reverse<br />
transcriptase inhibitor<br />
Three nucleoside reverse<br />
transcriptase inhibitors<br />
e.g. ZDV 3-TC or<br />
FTC Lop/rit<br />
e.g. ZDV or TDF 3-TC or<br />
FTC Efav or Nvp<br />
e.g. ABC ZDV 3-TC<br />
ABC, abacavir; ZDV, zidovudine; FTC, emtracitabine; 3-TC, 3-thiacytidine<br />
(lamivudine); d4T, didehydrothymidine (stavudine); Lop, lopinavir; rit,<br />
ritonovir; Efav, efavirenz; Nvp, nevirapine; TDF, tenofovir.<br />
a Combinations usually include ZDV or d4T because they have better CSF<br />
penetration than other nucleoside analogues <strong>and</strong> combinations attempt<br />
to avoid overlapping toxicities, <strong>and</strong> to avoid using agents that are<br />
phosphorylated by the same enzymes (combinations of ZDV d4T <strong>and</strong><br />
3-TC ddC are avoided. ddC 2 3-dideoxycytidine, also known as<br />
zalcitabine).<br />
specialist care. Current principles emphasize combination therapy,<br />
regime convenience, tolerability <strong>and</strong> lifelong therapy. Anti-<br />
HIV therapy is a complex therapeutic arena, necessitating<br />
specialist supervision.<br />
Key points<br />
General guidelines for anti-HIV-1 therapy<br />
• Treat before significant immunosuppression develops.<br />
• BHIVA treatment criteria are CD4 count (if 350/L) or<br />
symptoms or in USA HIV RNA 100,000 copies/mL plus<br />
CD4 350/L.<br />
• St<strong>and</strong>ard therapy is highly active antiretroviral therapy<br />
(HAART) combination therapy.<br />
• HAART is two nucleoside analogue inhibitors plus one<br />
protease inhibitor, e.g. ZDV 3-TC amprenavir (or<br />
lopinavir/ritonavir).<br />
• If there is drug treatment failure or resistance, change<br />
at least two <strong>and</strong> preferably all three drugs being used.<br />
• The revised regimen may be guided by genotyping of<br />
the HIV genome for mutations associated with drug<br />
resistance.<br />
ANTI-HIV DRUGS<br />
NUCLEOSIDE ANALOGUE REVERSE<br />
TRANSCRIPTASE INHIBITORS (NRTIs)<br />
Of these agents, only zidovudine (ZDV) has been proved to<br />
reduce mortality in late-stage AIDS. It reduces the incidence of<br />
opportunistic infections <strong>and</strong> possibly also the rate of progression<br />
of HIV-1 infection to AIDS. Other members of the class<br />
include lamivudine (3-TC), stavudine (d4T), didanosine<br />
(ddI), emtricitabine (FTC) <strong>and</strong> abacavir (ABC). These drugs<br />
are used in combinations <strong>and</strong> are available as combined<br />
products, e.g. 3-TC/ZDV, ABC/3-TC, ZDV/tenofovir. They<br />
reduce HIV-1 viral replication as indicated by plasma HIV<br />
RNA load.<br />
ZIDOVUDINE (AZIDOTHYMIDINE)<br />
This was originally synthesized in 1964 in the hope that it<br />
would be useful in treating malignancies. These hopes were<br />
not fulfilled, but it was the first nucleoside analogue effective<br />
in treating HIV-1 infection.<br />
Use<br />
Zidovudine (ZDV) is given orally to patients with HIV<br />
infection.<br />
Mechanism of action<br />
The parent drug, ZDV, enters virally infected cells by diffusion<br />
<strong>and</strong> undergoes phosphorylation first to its monophosphate<br />
(ZDV-MP) then to the diphosphate (ZDV-DP), the rate-limiting<br />
step, <strong>and</strong> finally to the triphosphate (ZDV-TP). The intracellular<br />
t 1/2 of ZDV-TP is two to three hours. ZDV-TP is a competitive<br />
inhibitor of the HIV-1 reverse transcriptase <strong>and</strong> when<br />
incorporated into nascent viral DNA causes chain termination.<br />
Human cells lack reverse transcriptase <strong>and</strong> human nuclear<br />
DNA polymerases are much less sensitive (by at least 100-fold)<br />
to inhibition by ZDV-TP, thus producing a selective effect on<br />
viral replication. This mechanism of action is common to all<br />
anti-HIV nucleoside analogues.<br />
Adverse effects<br />
These include the following:<br />
• dose-dependent bone marrow suppression causing<br />
anaemia with reticulocytopenia <strong>and</strong> granulocytopenia.<br />
This occurred in 15% of patients in the original studies<br />
with high-dose ZDV. At currently recommended doses, it<br />
occurs in only 1–2% of patients;<br />
• nausea <strong>and</strong> vomiting;<br />
• fatigue <strong>and</strong> headache;<br />
• melanonychia (blue-grey nail discoloration);<br />
• lipodystrophy;<br />
• mitochondrial myopathy (uncommon);<br />
• hepatic steatosis with lactic acidosis (rarely);<br />
• it is mutagenic <strong>and</strong> carcinogenic in animals. However,<br />
ZDV is used in HIV-positive pregnant women as it<br />
reduces HIV maternal–fetal transmission <strong>and</strong> thus<br />
fetal/neonatal HIV-1 infection <strong>and</strong> has not been shown to<br />
be teratogenic if given to women after the first trimester.<br />
Pharmacokinetics<br />
Zidovudine is almost totally absorbed (90%) from the<br />
gastro-intestinal tract, it achieves cerebrospinal fluid (CSF)<br />
concentrations that are 50% of those in plasma. The ZDV<br />
plasma elimination t 1/2 is one to two hours. About 25–40% of<br />
a dose undergoes presystemic metabolism in the liver. The<br />
major metabolite (80%) is the glucuronide <strong>and</strong> approximately<br />
20% of a dose appears unchanged in the urine.

