

Clinical Pharmacology and Therapeutics
A Textbook of Clinical Pharmacology and ... - clinicalevidence
A Textbook of Clinical Pharmacology and ... - clinicalevidence
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
370 CANCER CHEMOTHERAPY<br />
Table 48.2: Multiple mechanisms of acquired tumour drug resistance<br />
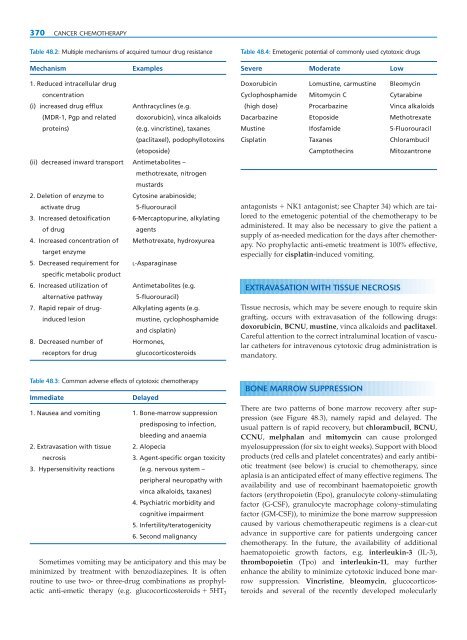
Table 48.4: Emetogenic potential of commonly used cytotoxic drugs<br />
Mechanism<br />
Examples<br />
Severe Moderate Low<br />
1. Reduced intracellular drug<br />
concentration<br />
(i) increased drug efflux Anthracyclines (e.g.<br />
(MDR-1, Pgp <strong>and</strong> related doxorubicin), vinca alkaloids<br />
proteins)<br />
(e.g. vincristine), taxanes<br />
(paclitaxel), podophyllotoxins<br />
(etoposide)<br />
(ii) decreased inward transport Antimetabolites –<br />
methotrexate, nitrogen<br />
mustards<br />
2. Deletion of enzyme to Cytosine arabinoside;<br />
activate drug<br />
5-fluorouracil<br />
3. Increased detoxification 6-Mercaptopurine, alkylating<br />
of drug<br />
agents<br />
4. Increased concentration of Methotrexate, hydroxyurea<br />
target enzyme<br />
5. Decreased requirement for L-Asparaginase<br />
specific metabolic product<br />
6. Increased utilization of Antimetabolites (e.g.<br />
alternative pathway<br />
5-fluorouracil)<br />
7. Rapid repair of drug- Alkylating agents (e.g.<br />
induced lesion<br />
mustine, cyclophosphamide<br />
<strong>and</strong> cisplatin)<br />
8. Decreased number of Hormones,<br />
receptors for drug<br />
glucocorticosteroids<br />
Doxorubicin Lomustine, carmustine Bleomycin<br />
Cyclophosphamide Mitomycin C Cytarabine<br />
(high dose) Procarbazine Vinca alkaloids<br />
Dacarbazine Etoposide Methotrexate<br />
Mustine Ifosfamide 5-Fluorouracil<br />
Cisplatin Taxanes Chlorambucil<br />
Camptothecins<br />
Mitozantrone<br />
antagonists NK1 antagonist; see Chapter 34) which are tailored<br />
to the emetogenic potential of the chemotherapy to be<br />
administered. It may also be necessary to give the patient a<br />
supply of as-needed medication for the days after chemotherapy.<br />
No prophylactic anti-emetic treatment is 100% effective,<br />
especially for cisplatin-induced vomiting.<br />
EXTRAVASATION WITH TISSUE NECROSIS<br />
Tissue necrosis, which may be severe enough to require skin<br />
grafting, occurs with extravasation of the following drugs:<br />
doxorubicin, BCNU, mustine, vinca alkaloids <strong>and</strong> paclitaxel.<br />
Careful attention to the correct intraluminal location of vascular<br />
catheters for intravenous cytotoxic drug administration is<br />
m<strong>and</strong>atory.<br />
Table 48.3: Common adverse effects of cytotoxic chemotherapy<br />
Immediate<br />
Delayed<br />
1. Nausea <strong>and</strong> vomiting 1. Bone-marrow suppression<br />
predisposing to infection,<br />
bleeding <strong>and</strong> anaemia<br />
2. Extravasation with tissue 2. Alopecia<br />
necrosis<br />
3. Agent-specific organ toxicity<br />
3. Hypersensitivity reactions (e.g. nervous system –<br />
peripheral neuropathy with<br />
vinca alkaloids, taxanes)<br />
4. Psychiatric morbidity <strong>and</strong><br />
cognitive impairment<br />
5. Infertility/teratogenicity<br />
6. Second malignancy<br />
Sometimes vomiting may be anticipatory <strong>and</strong> this may be<br />
minimized by treatment with benzodiazepines. It is often<br />
routine to use two- or three-drug combinations as prophylactic<br />
anti-emetic therapy (e.g. glucocorticosteroids 5HT 3<br />
BONE MARROW SUPPRESSION<br />
There are two patterns of bone marrow recovery after suppression<br />
(see Figure 48.3), namely rapid <strong>and</strong> delayed. The<br />
usual pattern is of rapid recovery, but chlorambucil, BCNU,<br />
CCNU, melphalan <strong>and</strong> mitomycin can cause prolonged<br />
myelosuppression (for six to eight weeks). Support with blood<br />
products (red cells <strong>and</strong> platelet concentrates) <strong>and</strong> early antibiotic<br />
treatment (see below) is crucial to chemotherapy, since<br />
aplasia is an anticipated effect of many effective regimens. The<br />
availability <strong>and</strong> use of recombinant haematopoietic growth<br />
factors (erythropoietin (Epo), granulocyte colony-stimulating<br />
factor (G-CSF), granulocyte macrophage colony-stimulating<br />
factor (GM-CSF)), to minimize the bone marrow suppression<br />
caused by various chemotherapeutic regimens is a clear-cut<br />
advance in supportive care for patients undergoing cancer<br />
chemotherapy. In the future, the availability of additional<br />
haematopoietic growth factors, e.g. interleukin-3 (IL-3),<br />
thrombopoietin (Tpo) <strong>and</strong> interleukin-11, may further<br />
enhance the ability to minimize cytotoxic induced bone marrow<br />
suppression. Vincristine, bleomycin, glucocorticosteroids<br />
<strong>and</strong> several of the recently developed molecularly

