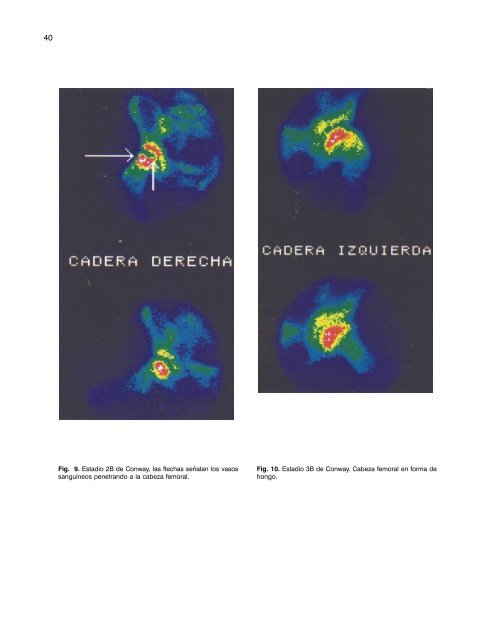
40 Fig. 9. Estadio 2B de Conway, las flechas señalan los vasos sanguíneos penetrando a la cabeza femoral. Fig. 10. Estadio 3B de Conway. Cabeza femoral en forma de hongo.
Fig. 11. Estadio 4B de Conway. Summary Bone scintigraphy with pinhole collimator and the classification derived from its utilization in the study of the Legg-Calvé-Perthes disease is introduced in our environment. 227 patients with presuntive diagnosis of this disease underwent scintigraphy at the Nuclear Medicine Department of the “Frank País” International Scientific Orthopedic Complex from September, 1996, to December, 1997 (including both). The diagnosis was confirmed in 28 cases (9 with normal X-rays) and other 31 affections were diagnosed. The relationship between radiography and scintigraphy was established, allowing to have a prognosis of the affection. Subject headings: LEGG-PERTHES DISEASE/pathology; GAMMA CAMERAS/utilization; DIAGNOSTIC IMAGING; EQUIPMENT AND SUPPLIES. Résumé Dans notre environnement, la gammagraphie osseuse avec collimateur pinhole, et la classification dérivée de son usage, sont introduites dans l’étude de la maladie de Legg-Calvé- Perthes. Elle a été pratiquée à 227 patients qui sont allés au Département de Médecine nucléaire du CSOI "Frank País" avec le diagnostic présumé de cette maladie, entre septembre 1996 et décembre 1997 (tous les deux). Le diagnostic a été confirmé en 28 cas (9 clichés normaux), et d’autres 31 affections se sont diagnostiquées. Le rapport entre la radiographie et la gammagraphie a été établi, permettant d’émettre un pronostic de l’affection. Mots clés: MALADIE DE LEGG-PERTHES/pathologie; CHAMBRES GAMMA/usage; DIAGNOSTIC PAR IMAGE, EQUIPEMENTS ET FOURNITURES. Referencias bibliográficas 1. Legg AT. An obscure affection of the hip joint. Boston Med Surg J 1910;162:202-4. 2. Calvé J. Sur une forme particulière de pseudo-coxalgie greffèe sur des deformations caracteristiques de I’extremite superieure du femur. Revue de Chirurgie 1910;30:54-84. 3. Perthes GC. Uber arthritis deformans juvenilis. Dtsch Z Chir 1910;107:111-59. 4. Tsao AK, Dias LS, Conway JJ, Straka P. The prognostic value and significance of serial bone scintigraphy in Legg- Calvè Perthes disease. J Pediatr Orthop 1997;17:230-9. 5. Catterall A. Adolescent hip pain after Perthes disease. Clin Orthop 1986;209:65-9. 6. Tachdjian MO. Ortopedia Pediátrica. 2 ed. Ciudad México, Interamericana 1994:1008-69. 7. Danigelis JA, Fisher RL, Ozonoff MB, Sziklas JJ. 99m Tc- Polyphosphate bone imaging in Legg-Perthes disease. Radiology 1975;115:407-13. 8. Waldenström H. The fist stage of coxa plana. Acta Orthop Scand 1934;5:1-34. 9. Catterall A. Legg-Calvè-Perthes syndrome. Clin Orthop 1981;158:41-52. 10. Salter RB, Thompson GH. Legg-Calvé-Perthes disease: the prognostic significance of the subcondrial fracture and a two group classification of the femoral head involvement. J Bone Joint Surg 1984;66-A:479-89. 11. Salter RB. Experimental and clinical aspects of Perthes disease. J Bone Joint Surg 1966;48-B:393-4. 12. Stulberg SD, Cooperman DR, Wallensten R. The natural history of Legg-Calvè-Perthes disease. J Bone Joint Surg 1981;63-A:1095-108. 13. Mose K. Methods of measuring in Legg-Calvè-Perthes disease with special regard to the prognosis. Clin Orthop 1980;150:103-9. 14. Herring JA, Neustadt JB, Williams JJ, Early SJ, Browne RH. The lateral pillar classification of Legg-Calvè-Perthes disease. J Pediatr Orthop 1992;12:143-50. 15. Conway JJ. A scintigraphy classification of Legg-Calvè- Perthes disease. Sem Nucl Med 1993;23:274-95. 16. Danigelis JA. Pinhole imaging in Legg-Calvé-Perthes: further observations. Sem Nucl Med 1976;6:69-82. 17. Lamont RL, Muz J, Herilbronner D, Bouwhuis JA. Quantitative assessment of femoral head involvement in Legg-Calvè- Perthes disease. J Bone Joint Surg 1981;63-A:746-52. 41
- Page 1 and 2: R R E E V V I I S S T T A A C C U U
- Page 3 and 4: Fijación externa de la técnica de
- Page 5 and 6: EDITORIAL Este número de nuestra r
- Page 7 and 8: sensibles pero poco específicos; h
- Page 9 and 10: Fig. 1. Relación sexo-edad en tumo
- Page 11 and 12: Fig. 5-a. Sarcoma sinovial. Radiogr
- Page 13 and 14: Fig. 6. Sarcoma indiferenciado del
- Page 15 and 16: de una quimioterapia para su admini
- Page 17 and 18: Referencias bibliográficas 1. Wats
- Page 19 and 20: COMPLEJO CIENTÍFICO ORTOPÉDICO IN
- Page 21 and 22: (Tumores óseos: Tratamiento y resu
- Page 23 and 24: No obstante ser el más empleado y
- Page 25 and 26: Todos los quistes femorales se frac
- Page 27 and 28: HOSPITAL MILITAR CENTRAL “DR. CAR
- Page 29 and 30: eferida por los pacientes de nuestr
- Page 31 and 32: COMPLEJO CIENTÍFICO ORTOPÉDICO IN
- Page 33 and 34: Clasificaciones a) Clasificación g
- Page 35 and 36: La tabla 2 nos muestra la agrupaci
- Page 37 and 38: Fig. 3a. El estudio con el colimado
- Page 39: Fig. 6. Paciente con enfermedad de
- Page 43 and 44: HOSPITAL PEDIÁTRICO PROVINCIAL “
- Page 45 and 46: Existen 2 principios diferentes de
- Page 47 and 48: HOSPITAL PEDIÁTRICO PROVINCIAL “
- Page 49 and 50: Fig. 2. Modo de acción tipo II. 4.
- Page 51 and 52: Pronóstico · Elevada mortalidad:
- Page 53 and 54: 5. Corral Pazos de Provens O, Rubio
- Page 55 and 56: Fernández y otros, en investigaci
- Page 57 and 58: Summary A retrospective study of th
- Page 59 and 60: gentilmente de flexionarlo, retroce
- Page 61 and 62: TABLA 1. Análisis de la influencia
- Page 63 and 64: Résumé Deux cent patients, ayant
- Page 65 and 66: con compresión transversal de la c
- Page 67 and 68: los espacios L4-L5 y L5-S1, 3 con l
- Page 69 and 70: HOSPITAL GENERAL DE MORÓN CIEGO DE
- Page 71 and 72: Fig. 1. Anestesia empleada. La figu
- Page 73 and 74: Complejo Científico Ortopédico In
- Page 75 and 76: TABLA 4. Tipo de fractura de claví
- Page 77 and 78: HOSPITAL CLINICOQUIRÚRGICO “JOAQ
- Page 79 and 80: 6. Osteoartritis de la articulació
- Page 81 and 82: Con la modificación de Fitzgerald
- Page 83 and 84: CLÍNICA DE MEDICINA NATURAL Y TRAD
- Page 85 and 86: Similitud en la acción terapéutic
- Page 87 and 88: · Mejorado: Disminución ostensibl
- Page 89 and 90: inflamación pélvica, prostatitis,
- Page 91 and 92:
otros 13,14 también reportan bueno
- Page 93 and 94:
Fig. 2. Complicaciones. 3 Fig. 3. E
- Page 95 and 96:
COMPLEJO CIENTÍFICO ORTOPÉDICO IN
- Page 97 and 98:
Haddad y Riordan, también han surg
- Page 99 and 100:
INSTITUTO SUPERIOR DE MEDICINA MILI
- Page 101 and 102:
Fig.1c. Resultado final. Tejido ós
- Page 103 and 104:
Referencias bibliográficas 1. Ceba
- Page 105 and 106:
las uñas pueden ser bífidas, hemi
- Page 107 and 108:
Summary A patient with multiple con
- Page 109 and 110:
ocasión, dolor, aumento de volumen
- Page 111 and 112:
2. Huvos AG. Tumores óseos: diagn
- Page 113 and 114:
EXÁMENES COMPLEMENTARIOS - Hemoglo
- Page 115 and 116:
HOSPITAL PROVINCIAL DOCENTE “DR.
- Page 117 and 118:
Fig. 2. Miembros inferiores deforma
- Page 119 and 120:
COMPLEJO CIENTÍFICO ORTOPÉDICO IN
- Page 121 and 122:
Paciente masculino de 7 años de ed
- Page 123 and 124:
COMPLEJO CIENTÍFICO ORTOPÉDICO IN
- Page 125 and 126:
fémur (epifiso-metafisaria), toma
- Page 127 and 128:
supracondílea del fémur derecho y
- Page 129 and 130:
HOSPITAL PEDIÁTRICO DOCENTE “ELI
- Page 131 and 132:
Fig. 3. Rayos X de ambos pies (vist
- Page 133 and 134:
En este sentido, la hidroxiapatita
- Page 135 and 136:
Fig. 4. Evaluación cualitativa de
- Page 137 and 138:
HOSPITAL MILITAR CENTRAL “DR. CAR
- Page 139 and 140:
La complicación más importante es
- Page 141:
Revista Cubana de Ortopedia y Traum