

CHAPTER X CHAPTER 4 - Cancer et environnement
CHAPTER X CHAPTER 4 - Cancer et environnement
CHAPTER X CHAPTER 4 - Cancer et environnement

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
A<br />
B<br />
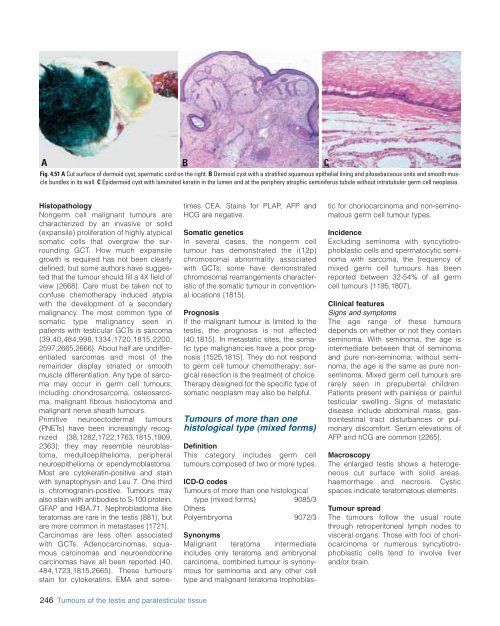
Fig. 4.51 A Cut surface of dermoid cyst, spermatic cord on the right. B Dermoid cyst with a stratified squamous epithelial lining and pilosebaceous units and smooth muscle<br />
bundles in its wall. C Epidermoid cyst with laminated keratin in the lumen and at the periphery atrophic seminiferus tubule without intratubuler germ cell neoplasia.<br />
C<br />
Histopathology<br />
Nongerm cell malignant tumours are<br />
characterized by an invasive or solid<br />
(expansile) proliferation of highly atypical<br />
somatic cells that overgrow the surrounding<br />
GCT. How much expansile<br />
growth is required has not been clearly<br />
defined, but some authors have suggested<br />
that the tumour should fill a 4X field of<br />
view {2668}. Care must be taken not to<br />
confuse chemotherapy induced atypia<br />
with the development of a secondary<br />
malignancy. The most common type of<br />
somatic type malignancy seen in<br />
patients with testicular GCTs is sarcoma<br />
{39,40,484,998,1334,1720,1815,2200,<br />
2597,2665,2666}. About half are undifferentiated<br />
sarcomas and most of the<br />
remainder display striated or smooth<br />
muscle differentiation. Any type of sarcoma<br />
may occur in germ cell tumours,<br />
including chondrosarcoma, osteosarcoma,<br />
malignant fibrous histiocytoma and<br />
malignant nerve sheath tumours.<br />
Primitive neuroectodermal tumours<br />
(PNETs) have been increasingly recognized<br />
{38,1282,1722,1763,1815,1909,<br />
2363}; they may resemble neuroblastoma,<br />
medulloepithelioma, peripheral<br />
neuroepithelioma or ependymoblastoma.<br />
Most are cytokeratin-positive and stain<br />
with synaptophysin and Leu 7. One third<br />
is chromogranin-positive. Tumours may<br />
also stain with antibodies to S-100 protein,<br />
GFAP and HBA.71. Nephroblastoma like<br />
teratomas are rare in the testis {881}, but<br />
are more common in m<strong>et</strong>astases {1721}.<br />
Carcinomas are less often associated<br />
with GCTs. Adenocarcinomas, squamous<br />
carcinomas and neuroendocrine<br />
carcinomas have all been reported {40,<br />
484,1723,1815,2665}. These tumours<br />
stain for cytokeratins, EMA and som<strong>et</strong>imes<br />
CEA. Stains for PLAP, AFP and<br />
HCG are negative.<br />
Somatic gen<strong>et</strong>ics<br />
In several cases, the nongerm cell<br />
tumour has demonstrated the i(12p)<br />
chromosomal abnormality associated<br />
with GCTs; some have demonstrated<br />
chromosomal rearrangements characteristic<br />
of the somatic tumour in conventional<br />
locations {1815}.<br />
Prognosis<br />
If the malignant tumour is limited to the<br />
testis, the prognosis is not affected<br />
{40,1815}. In m<strong>et</strong>astatic sites, the somatic<br />
type malignancies have a poor prognosis<br />
{1525,1815}. They do not respond<br />
to germ cell tumour chemotherapy; surgical<br />
resection is the treatment of choice.<br />
Therapy designed for the specific type of<br />
somatic neoplasm may also be helpful.<br />
Tumours of more than one<br />
histological type (mixed forms)<br />
Definition<br />
This category includes germ cell<br />
tumours composed of two or more types.<br />
ICD-O codes<br />
Tumours of more than one histological<br />
type (mixed forms) 9085/3<br />
Others<br />
Polyembryoma 9072/3<br />
Synonyms<br />
Malignant teratoma intermediate<br />
includes only teratoma and embryonal<br />
carcinoma, combined tumour is synonymous<br />
for seminoma and any other cell<br />
type and malignant teratoma trophoblastic<br />
for choriocarcinoma and non-seminomatous<br />
germ cell tumour types.<br />
Incidence<br />
Excluding seminoma with syncytiotrophoblastic<br />
cells and spermatocytic seminoma<br />
with sarcoma, the frequency of<br />
mixed germ cell tumours has been<br />
reported b<strong>et</strong>ween 32-54% of all germ<br />
cell tumours {1195,1807}.<br />
Clinical features<br />
Signs and symptoms<br />
The age range of these tumours<br />
depends on wh<strong>et</strong>her or not they contain<br />
seminoma. With seminoma, the age is<br />
intermediate b<strong>et</strong>ween that of seminoma<br />
and pure non-seminoma; without seminoma,<br />
the age is the same as pure nonseminoma.<br />
Mixed germ cell tumours are<br />
rarely seen in prepubertal children.<br />
Patients present with painless or painful<br />
testicular swelling. Signs of m<strong>et</strong>astatic<br />
disease include abdominal mass, gastrointestinal<br />
tract disturbances or pulmonary<br />
discomfort. Serum elevations of<br />
AFP and hCG are common {2265}.<br />
Macroscopy<br />
The enlarged testis shows a h<strong>et</strong>erogeneous<br />
cut surface with solid areas,<br />
haemorrhage and necrosis. Cystic<br />
spaces indicate teratomatous elements.<br />
Tumour spread<br />
The tumours follow the usual route<br />
through r<strong>et</strong>roperitoneal lymph nodes to<br />
visceral organs. Those with foci of choriocarcinoma<br />
or numerous syncytiotrophoblastic<br />
cells tend to involve liver<br />
and/or brain.<br />
246 Tumours of the testis and paratesticular tissue













