

A-Textbook-of-Clinical-Pharmacology-and-Therapeutics-5th-edition
A-Textbook-of-Clinical-Pharmacology-and-Therapeutics-5th-edition
A-Textbook-of-Clinical-Pharmacology-and-Therapeutics-5th-edition

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
188 HYPERTENSION<br />
Angiotensin receptor<br />
blocker<br />
Vasoconstriction<br />
<br />
Angiotensinogen<br />
Cell<br />
growth<br />
Angiotensin I<br />
Angiotensin II<br />
AT 1 -receptor<br />
Sodium <strong>and</strong><br />
fluid<br />
retention<br />
Renin<br />
ACE<br />
ACE inhibitor<br />
Sympathetic<br />
activation<br />
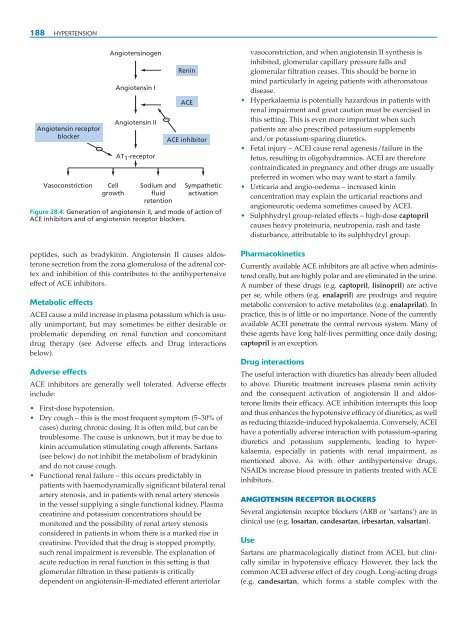
Figure 28.4: Generation <strong>of</strong> angiotensin II, <strong>and</strong> mode <strong>of</strong> action <strong>of</strong><br />
ACE inhibitors <strong>and</strong> <strong>of</strong> angiotensin receptor blockers.<br />
peptides, such as bradykinin. Angiotensin II causes aldosterone<br />
secretion from the zona glomerulosa <strong>of</strong> the adrenal cortex<br />
<strong>and</strong> inhibition <strong>of</strong> this contributes to the antihypertensive<br />
effect <strong>of</strong> ACE inhibitors.<br />
Metabolic effects<br />
ACEI cause a mild increase in plasma potassium which is usually<br />
unimportant, but may sometimes be either desirable or<br />
problematic depending on renal function <strong>and</strong> concomitant<br />
drug therapy (see Adverse effects <strong>and</strong> Drug interactions<br />
below).<br />
Adverse effects<br />
ACE inhibitors are generally well tolerated. Adverse effects<br />
include:<br />
• First-dose hypotension.<br />
• Dry cough – this is the most frequent symptom (5–30% <strong>of</strong><br />
cases) during chronic dosing. It is <strong>of</strong>ten mild, but can be<br />
troublesome. The cause is unknown, but it may be due to<br />
kinin accumulation stimulating cough afferents. Sartans<br />
(see below) do not inhibit the metabolism <strong>of</strong> bradykinin<br />
<strong>and</strong> do not cause cough.<br />
• Functional renal failure – this occurs predictably in<br />
patients with haemodynamically significant bilateral renal<br />
artery stenosis, <strong>and</strong> in patients with renal artery stenosis<br />
in the vessel supplying a single functional kidney. Plasma<br />
creatinine <strong>and</strong> potassium concentrations should be<br />
monitored <strong>and</strong> the possibility <strong>of</strong> renal artery stenosis<br />
considered in patients in whom there is a marked rise in<br />
creatinine. Provided that the drug is stopped promptly,<br />
such renal impairment is reversible. The explanation <strong>of</strong><br />
acute reduction in renal function in this setting is that<br />
glomerular filtration in these patients is critically<br />
dependent on angiotensin-II-mediated efferent arteriolar<br />
<br />
vasoconstriction, <strong>and</strong> when angiotensin II synthesis is<br />
inhibited, glomerular capillary pressure falls <strong>and</strong><br />
glomerular filtration ceases. This should be borne in<br />
mind particularly in ageing patients with atheromatous<br />
disease.<br />
• Hyperkalaemia is potentially hazardous in patients with<br />
renal impairment <strong>and</strong> great caution must be exercised in<br />
this setting. This is even more important when such<br />
patients are also prescribed potassium supplements<br />
<strong>and</strong>/or potassium-sparing diuretics.<br />
• Fetal injury – ACEI cause renal agenesis/failure in the<br />
fetus, resulting in oligohydramnios. ACEI are therefore<br />
contraindicated in pregnancy <strong>and</strong> other drugs are usually<br />
preferred in women who may want to start a family.<br />
• Urticaria <strong>and</strong> angio-oedema – increased kinin<br />
concentration may explain the urticarial reactions <strong>and</strong><br />
angioneurotic oedema sometimes caused by ACEI.<br />
• Sulphhydryl group-related effects – high-dose captopril<br />
causes heavy proteinuria, neutropenia, rash <strong>and</strong> taste<br />
disturbance, attributable to its sulphhydryl group.<br />
Pharmacokinetics<br />
Currently available ACE inhibitors are all active when administered<br />
orally, but are highly polar <strong>and</strong> are eliminated in the urine.<br />
A number <strong>of</strong> these drugs (e.g. captopril, lisinopril) are active<br />
per se, while others (e.g. enalapril) are prodrugs <strong>and</strong> require<br />
metabolic conversion to active metabolites (e.g. enalaprilat). In<br />
practice, this is <strong>of</strong> little or no importance. None <strong>of</strong> the currently<br />
available ACEI penetrate the central nervous system. Many <strong>of</strong><br />
these agents have long half-lives permitting once daily dosing;<br />
captopril is an exception.<br />
Drug interactions<br />
The useful interaction with diuretics has already been alluded<br />
to above. Diuretic treatment increases plasma renin activity<br />
<strong>and</strong> the consequent activation <strong>of</strong> angiotensin II <strong>and</strong> aldosterone<br />
limits their efficacy. ACE inhibition interrupts this loop<br />
<strong>and</strong> thus enhances the hypotensive efficacy <strong>of</strong> diuretics, as well<br />
as reducing thiazide-induced hypokalaemia. Conversely, ACEI<br />
have a potentially adverse interaction with potassium-sparing<br />
diuretics <strong>and</strong> potassium supplements, leading to hyperkalaemia,<br />
especially in patients with renal impairment, as<br />
mentioned above. As with other antihypertensive drugs,<br />
NSAIDs increase blood pressure in patients treated with ACE<br />
inhibitors.<br />
ANGIOTENSIN RECEPTOR BLOCKERS<br />
Several angiotensin receptor blockers (ARB or ‘sartans’) are in<br />
clinical use (e.g. losartan, c<strong>and</strong>esartan, irbesartan, valsartan).<br />
Use<br />
Sartans are pharmacologically distinct from ACEI, but clinically<br />
similar in hypotensive efficacy. However, they lack the<br />
common ACEI adverse effect <strong>of</strong> dry cough. Long-acting drugs<br />
(e.g. c<strong>and</strong>esartan, which forms a stable complex with the