

A-Textbook-of-Clinical-Pharmacology-and-Therapeutics-5th-edition
A-Textbook-of-Clinical-Pharmacology-and-Therapeutics-5th-edition
A-Textbook-of-Clinical-Pharmacology-and-Therapeutics-5th-edition

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
222 CARDIAC DYSRHYTHMIAS<br />
• Support ABCs; give oxygen; cannulate a vein<br />
• Monitor ECG, BP, SpO 2<br />
• Record 12-lead if possible, if not record rhythm strip<br />
• Identify <strong>and</strong> treat reversible causes<br />
Synchronised DC shock*<br />
up to 3 attempts<br />
• Amiodarone 300 mg IV over 10–20<br />
min <strong>and</strong> repeat shock; followed by;<br />
• Amiodarone 900 mg over 24 h<br />
Irregular<br />
Seek expert help<br />
Possibilities include:<br />
• AF with bundle branch block<br />
treat as for narrow complex<br />
• Pre-excited AF<br />
consider amiodarone<br />
• Polymorphic VT (e.g.<br />
torsades de pointes – give<br />
magnesium 2 g over 10 min)<br />
Unstable<br />
Is QRS regular<br />
*Attempted electrical cardioversion is<br />
always undertaken under sedation<br />
or general anaesthesia<br />
Broad<br />
Is patient stable<br />
Signs <strong>of</strong> instability include:<br />
1. Reduced conscious level 2. Chest pain<br />
3. Systolic BP 90 mmHg 4. Heart failure<br />
(Rate related symptoms uncommon at less<br />
than 150 beats min 1 )<br />
Regular<br />
Stable<br />
Is QRS narrow (0.12 sec)<br />
If ventricular tachycardia<br />
(or uncertain rhythm):<br />
• Amiodarone 300 mg IV<br />
over 20–60 min; then 900 mg<br />
over 24 h<br />
If previously confirmed SVT<br />
with bundle branch block:<br />
• Give adenosine as for regular<br />
narrow complex tachycardia<br />
Regular<br />
Narrow<br />
• Use vagal manoeuvres<br />
• Adenosine 6 mg rapid IV bolus;<br />
if unsuccessful give 12 mg;<br />
if unsuccessful give futher 12 mg.<br />
• Monitor ECG continuously<br />
Normal sinus rhythm<br />
restored<br />
Yes<br />
Probable re-entry PSVT:<br />
• Record 12-lead ECG in<br />
sinus rhythm<br />
• If recurs, give adenosine<br />
again & consider choice <strong>of</strong><br />
anti-dyshythmic prophylaxis<br />
Is rhythm regular<br />
Irregular<br />
Irregular narrow complex<br />
tachycardia<br />
Probable atrial fibrillation<br />
Control rate with:<br />
• β-Blocker IV, digoxin IV, or<br />
diltiazem IV<br />
if onset 48 h consider:<br />
• Amiodarone 300 mg IV 20–60<br />
min; then 900 mg over 24 h<br />
No<br />
Seek expert help<br />
Possible atrial flutter<br />
• Control rate (e.g. β-Blocker)<br />
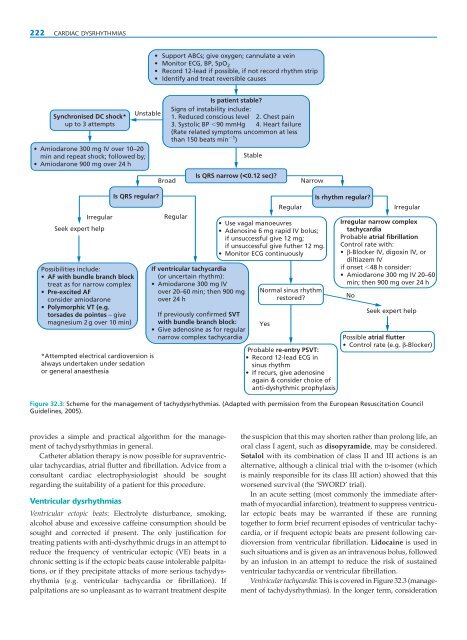
Figure 32.3: Scheme for the management <strong>of</strong> tachydysrhythmias. (Adapted with permission from the European Resuscitation Council<br />
Guidelines, 2005).<br />
provides a simple <strong>and</strong> practical algorithm for the management<br />
<strong>of</strong> tachydysrhythmias in general.<br />
Catheter ablation therapy is now possible for supraventricular<br />
tachycardias, atrial flutter <strong>and</strong> fibrillation. Advice from a<br />
consultant cardiac electrophysiologist should be sought<br />
regarding the suitability <strong>of</strong> a patient for this procedure.<br />
Ventricular dysrhythmias<br />
Ventricular ectopic beats: Electrolyte disturbance, smoking,<br />
alcohol abuse <strong>and</strong> excessive caffeine consumption should be<br />
sought <strong>and</strong> corrected if present. The only justification for<br />
treating patients with anti-dysrhythmic drugs in an attempt to<br />
reduce the frequency <strong>of</strong> ventricular ectopic (VE) beats in a<br />
chronic setting is if the ectopic beats cause intolerable palpitations,<br />
or if they precipitate attacks <strong>of</strong> more serious tachydysrhythmia<br />
(e.g. ventricular tachycardia or fibrillation). If<br />
palpitations are so unpleasant as to warrant treatment despite<br />
the suspicion that this may shorten rather than prolong life, an<br />
oral class I agent, such as disopyramide, may be considered.<br />
Sotalol with its combination <strong>of</strong> class II <strong>and</strong> III actions is an<br />
alternative, although a clinical trial with the D-isomer (which<br />
is mainly responsible for its class III action) showed that this<br />
worsened survival (the ‘SWORD’ trial).<br />
In an acute setting (most commonly the immediate aftermath<br />
<strong>of</strong> myocardial infarction), treatment to suppress ventricular<br />
ectopic beats may be warranted if these are running<br />
together to form brief recurrent episodes <strong>of</strong> ventricular tachycardia,<br />
or if frequent ectopic beats are present following cardioversion<br />
from ventricular fibrillation. Lidocaine is used in<br />
such situations <strong>and</strong> is given as an intravenous bolus, followed<br />
by an infusion in an attempt to reduce the risk <strong>of</strong> sustained<br />
ventricular tachycardia or ventricular fibrillation.<br />
Ventricular tachycardia: This is covered in Figure 32.3 (management<br />
<strong>of</strong> tachydysrhythmias). In the longer term, consideration