

A-Textbook-of-Clinical-Pharmacology-and-Therapeutics-5th-edition
A-Textbook-of-Clinical-Pharmacology-and-Therapeutics-5th-edition
A-Textbook-of-Clinical-Pharmacology-and-Therapeutics-5th-edition

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
250 ALIMENTARY SYSTEM AND LIVER<br />
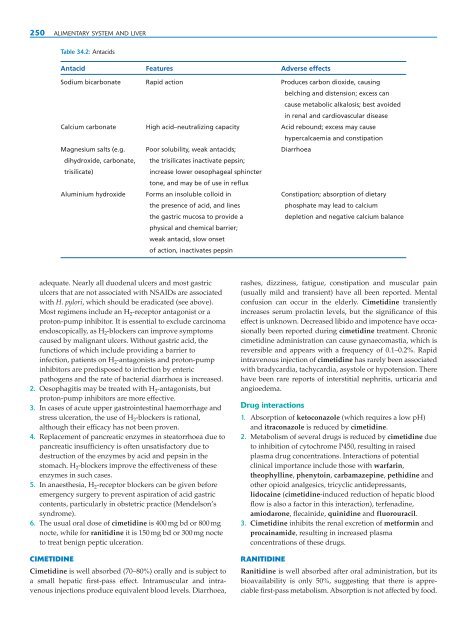
Table 34.2: Antacids<br />
Antacid Features Adverse effects<br />
Sodium bicarbonate Rapid action Produces carbon dioxide, causing<br />
belching <strong>and</strong> distension; excess can<br />
cause metabolic alkalosis; best avoided<br />
in renal <strong>and</strong> cardiovascular disease<br />
Calcium carbonate High acid–neutralizing capacity Acid rebound; excess may cause<br />
hypercalcaemia <strong>and</strong> constipation<br />
Magnesium salts (e.g. Poor solubility, weak antacids; Diarrhoea<br />
dihydroxide, carbonate, the trisilicates inactivate pepsin;<br />
trisilicate)<br />
increase lower oesophageal sphincter<br />
tone, <strong>and</strong> may be <strong>of</strong> use in reflux<br />
Aluminium hydroxide Forms an insoluble colloid in Constipation; absorption <strong>of</strong> dietary<br />
the presence <strong>of</strong> acid, <strong>and</strong> lines<br />
phosphate may lead to calcium<br />
the gastric mucosa to provide a<br />
depletion <strong>and</strong> negative calcium balance<br />
physical <strong>and</strong> chemical barrier;<br />
weak antacid, slow onset<br />
<strong>of</strong> action, inactivates pepsin<br />
adequate. Nearly all duodenal ulcers <strong>and</strong> most gastric<br />
ulcers that are not associated with NSAIDs are associated<br />
with H. pylori, which should be eradicated (see above).<br />
Most regimens include an H 2 -receptor antagonist or a<br />
proton-pump inhibitor. It is essential to exclude carcinoma<br />
endoscopically, as H 2 -blockers can improve symptoms<br />
caused by malignant ulcers. Without gastric acid, the<br />
functions <strong>of</strong> which include providing a barrier to<br />
infection, patients on H 2 -antagonists <strong>and</strong> proton-pump<br />
inhibitors are predisposed to infection by enteric<br />
pathogens <strong>and</strong> the rate <strong>of</strong> bacterial diarrhoea is increased.<br />
2. Oesophagitis may be treated with H 2 -antagonists, but<br />
proton-pump inhibitors are more effective.<br />
3. In cases <strong>of</strong> acute upper gastrointestinal haemorrhage <strong>and</strong><br />
stress ulceration, the use <strong>of</strong> H 2 -blockers is rational,<br />
although their efficacy has not been proven.<br />
4. Replacement <strong>of</strong> pancreatic enzymes in steatorrhoea due to<br />
pancreatic insufficiency is <strong>of</strong>ten unsatisfactory due to<br />
destruction <strong>of</strong> the enzymes by acid <strong>and</strong> pepsin in the<br />
stomach. H 2 -blockers improve the effectiveness <strong>of</strong> these<br />
enzymes in such cases.<br />
5. In anaesthesia, H 2 -receptor blockers can be given before<br />
emergency surgery to prevent aspiration <strong>of</strong> acid gastric<br />
contents, particularly in obstetric practice (Mendelson’s<br />
syndrome).<br />
6. The usual oral dose <strong>of</strong> cimetidine is 400 mg bd or 800 mg<br />
nocte, while for ranitidine it is 150 mg bd or 300 mg nocte<br />
to treat benign peptic ulceration.<br />
CIMETIDINE<br />
Cimetidine is well absorbed (70–80%) orally <strong>and</strong> is subject to<br />
a small hepatic first-pass effect. Intramuscular <strong>and</strong> intravenous<br />
injections produce equivalent blood levels. Diarrhoea,<br />
rashes, dizziness, fatigue, constipation <strong>and</strong> muscular pain<br />
(usually mild <strong>and</strong> transient) have all been reported. Mental<br />
confusion can occur in the elderly. Cimetidine transiently<br />
increases serum prolactin levels, but the significance <strong>of</strong> this<br />
effect is unknown. Decreased libido <strong>and</strong> impotence have occasionally<br />
been reported during cimetidine treatment. Chronic<br />
cimetidine administration can cause gynaecomastia, which is<br />
reversible <strong>and</strong> appears with a frequency <strong>of</strong> 0.1–0.2%. Rapid<br />
intravenous injection <strong>of</strong> cimetidine has rarely been associated<br />
with bradycardia, tachycardia, asystole or hypotension. There<br />
have been rare reports <strong>of</strong> interstitial nephritis, urticaria <strong>and</strong><br />
angioedema.<br />
Drug interactions<br />
1. Absorption <strong>of</strong> ketoconazole (which requires a low pH)<br />
<strong>and</strong> itraconazole is reduced by cimetidine.<br />
2. Metabolism <strong>of</strong> several drugs is reduced by cimetidine due<br />
to inhibition <strong>of</strong> cytochrome P450, resulting in raised<br />
plasma drug concentrations. Interactions <strong>of</strong> potential<br />
clinical importance include those with warfarin,<br />
theophylline, phenytoin, carbamazepine, pethidine <strong>and</strong><br />
other opioid analgesics, tricyclic antidepressants,<br />
lidocaine (cimetidine-induced reduction <strong>of</strong> hepatic blood<br />
flow is also a factor in this interaction), terfenadine,<br />
amiodarone, flecainide, quinidine <strong>and</strong> fluorouracil.<br />
3. Cimetidine inhibits the renal excretion <strong>of</strong> metformin <strong>and</strong><br />
procainamide, resulting in increased plasma<br />
concentrations <strong>of</strong> these drugs.<br />
RANITIDINE<br />
Ranitidine is well absorbed after oral administration, but its<br />
bioavailability is only 50%, suggesting that there is appreciable<br />
first-pass metabolism. Absorption is not affected by food.