

Vol 44 # 2 June 2012 - Kma.org.kw
Vol 44 # 2 June 2012 - Kma.org.kw
Vol 44 # 2 June 2012 - Kma.org.kw

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<strong>June</strong> <strong>2012</strong><br />
KUWAIT MEDICAL JOURNAL 122<br />
a history of neurologic or psychiatric disease,<br />
difficulty with communication, analgesic and / or<br />
sedative administration, history of renal or hepatic<br />
insufficiency, thrombophlebitis and hypersensitivity<br />
to the study drugs were excluded from the study.<br />
On patient arrival in the operating room without<br />
any premedication, a 22-gauge intravenous (IV)<br />
catheter was inserted into a vein on the dorsum<br />
of the hand. Patients were monitored with<br />
electrocardiography, pulse oximetry (oxygen<br />
saturation), and non-invasive blood pressure. All<br />
infusion fluids were 0.9% normal saline at a rate of 500<br />
ml/h. The study subjects were randomly allocated<br />
to one of four groups to receive either saline, 0.5, 1 or<br />
2 mcg sufentanil in 2 ml volume. Thirty seconds after<br />
the intravenous (IV) injection of the pretreatment<br />
drug, 5 ml of 1% propofol at room temperature<br />
(Fresenius Kabi, Hamburg, Germany) was injected<br />
IV at a rate of 0.5 ml/sec. Pain was assesed verbally<br />
and scored as none (0), mild (1), moderate (2) and<br />
severe (3). Any spontaneous complaints of pain were<br />
noted. If there were no spontaneous complaints,<br />
patients were asked about pain 30 seconds after the<br />
propofol injection. Observations were noted by an<br />
independent observer.<br />
Induction of anesthesia was performed in all<br />
patients with propofol upto 2.5 mg/kg, 0.6 mg/ kg<br />
atracurium and 1 - 2 mcg sufentanil. Anesthesia was<br />
maintained with nitrous oxide 50% and sevoflurane<br />
2 - 2.5% in oxygen.<br />
Any excitation during induction and reactions<br />
such as hypotension, nausea, vomiting or flushing<br />
were recorded.<br />
Statical analysis<br />
Statistical analysis was carried out using SPSS for<br />
WINDOWS software program version 15.0 (SPSS,<br />
Chicago, IL). The Mann Whitney-U test was used<br />
to analyze the results of the patients’ subjective<br />
assessment of pain. A p-value less than 0.05 was<br />
considered statistically significant. Differences<br />
between scores from the saline group and the other<br />
groups were estimated as 1.5 and with a 0.05 α error<br />
Table 1: Characteristics of the patients (mean ± SD)<br />
Patient<br />
Group 1 Group 2 Group 3 Group 4<br />
Characteristics<br />
Sex (F/M)<br />
ASA I/II<br />
Age<br />
Weight (kg)<br />
Status of Pain<br />
No Pain<br />
Pain<br />
17/23<br />
21/19<br />
37.8 ± 12.05<br />
70.2 ± 11.03<br />
Group 1<br />
%<br />
7.5<br />
92.5<br />
21/19<br />
19/21<br />
38.4 ± 13.10<br />
70.7 ± 12.08<br />
Group 2<br />
%<br />
5<br />
95<br />
19/21<br />
20/20<br />
34.08 ± 12.06<br />
70.97 ± 11.05<br />
Group 3<br />
%<br />
22.5<br />
77.5 *<br />
18/22<br />
21/19<br />
33.03 ± 11.04<br />
70.55 ± 12.7<br />
(two- sided) the required sample size was 40 per<br />
group yielding a power higher than 90%.<br />
RESULTS<br />
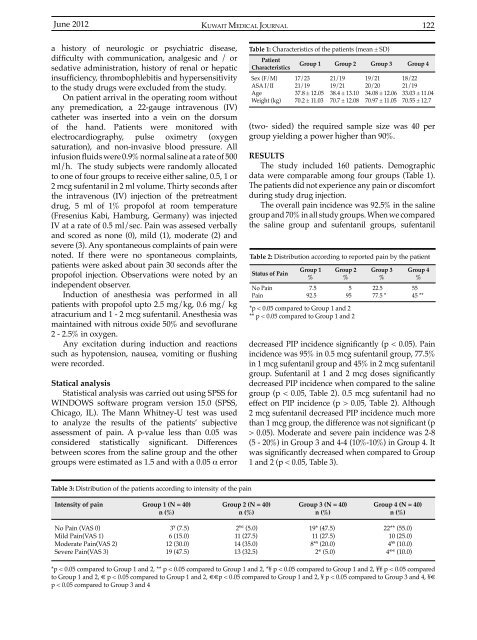
The study included 160 patients. Demographic<br />
data were comparable among four groups (Table 1).<br />
The patients did not experience any pain or discomfort<br />
during study drug injection.<br />
The overall pain incidence was 92.5% in the saline<br />
group and 70% in all study groups. When we compared<br />
the saline group and sufentanil groups, sufentanil<br />
Table 2: Distribution according to reported pain by the patient<br />
*p < 0.05 compared to Group 1 and 2<br />
** p < 0.05 compared to Group 1 and 2<br />
Group 4<br />
%<br />
55<br />
45 **<br />
decreased PIP incidence significantly (p < 0.05). Pain<br />
incidence was 95% in 0.5 mcg sufentanil group, 77.5%<br />
in 1 mcg sufentanil group and 45% in 2 mcg sufentanil<br />
group. Sufentanil at 1 and 2 mcg doses significantly<br />
decreased PIP incidence when compared to the saline<br />
group (p < 0.05, Table 2). 0.5 mcg sufentanil had no<br />
effect on PIP incidence (p > 0.05, Table 2). Although<br />
2 mcg sufentanil decreased PIP incidence much more<br />
than 1 mcg group, the difference was not significant (p<br />
> 0.05). Moderate and severe pain incidence was 2-8<br />
(5 - 20%) in Group 3 and 4-4 (10%-10%) in Group 4. It<br />
was significantly decreased when compared to Group<br />
1 and 2 (p < 0.05, Table 3).<br />
Table 3: Distribution of the patients according to intensity of the pain<br />
Intensity of pain<br />
Group 1 (N = 40)<br />
n (%)<br />
Group 2 (N = 40)<br />
n (%)<br />
Group 3 (N = 40)<br />
n (%)<br />
Group 4 (N = 40)<br />
n (%)<br />
No Pain (VAS 0)<br />
Mild Pain(VAS 1)<br />
Moderate Pain(VAS 2)<br />
Severe Pain(VAS 3)<br />
3 ¥ (7.5)<br />
6 (15.0)<br />
12 (30.0)<br />
19 (47.5)<br />
2 ¥€ (5.0)<br />
11 (27.5)<br />
14 (35.0)<br />
13 (32.5)<br />
19* (47.5)<br />
11 (27.5)<br />
8* ¥ (20.0)<br />
2 € (5.0)<br />
22** (55.0)<br />
10 (25.0)<br />
4 ¥¥ (10.0)<br />
4 €€ (10.0)<br />
*p < 0.05 compared to Group 1 and 2, ** p < 0.05 compared to Group 1 and 2, *¥ p < 0.05 compared to Group 1 and 2, ¥¥ p < 0.05 compared<br />
to Group 1 and 2, € p < 0.05 compared to Group 1 and 2, €€p < 0.05 compared to Group 1 and 2, ¥ p < 0.05 compared to Group 3 and 4, ¥€<br />
p < 0.05 compared to Group 3 and 4













