

Vol 44 # 2 June 2012 - Kma.org.kw
Vol 44 # 2 June 2012 - Kma.org.kw
Vol 44 # 2 June 2012 - Kma.org.kw

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<strong>June</strong> <strong>2012</strong><br />
KUWAIT MEDICAL JOURNAL 1<strong>44</strong><br />
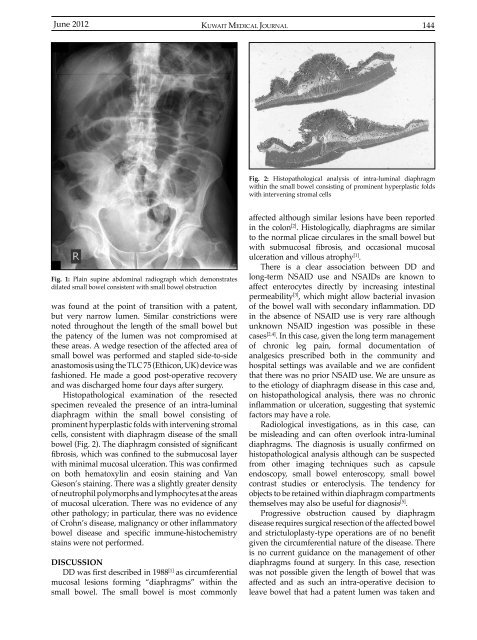
Fig. 2: Histopathological analysis of intra-luminal diaphragm<br />
within the small bowel consisting of prominent hyperplastic folds<br />
with intervening stromal cells<br />
Fig. 1: Plain supine abdominal radiograph which demonstrates<br />
dilated small bowel consistent with small bowel obstruction<br />
was found at the point of transition with a patent,<br />
but very narrow lumen. Similar constrictions were<br />
noted throughout the length of the small bowel but<br />
the patency of the lumen was not compromised at<br />
these areas. A wedge resection of the affected area of<br />
small bowel was performed and stapled side-to-side<br />
anastomosis using the TLC 75 (Ethicon, UK) device was<br />
fashioned. He made a good post-operative recovery<br />
and was discharged home four days after surgery.<br />
Histopathological examination of the resected<br />
specimen revealed the presence of an intra-luminal<br />
diaphragm within the small bowel consisting of<br />
prominent hyperplastic folds with intervening stromal<br />
cells, consistent with diaphragm disease of the small<br />
bowel (Fig. 2). The diaphragm consisted of significant<br />
fibrosis, which was confined to the submucosal layer<br />
with minimal mucosal ulceration. This was confirmed<br />
on both hematoxylin and eosin staining and Van<br />
Gieson’s staining. There was a slightly greater density<br />
of neutrophil polymorphs and lymphocytes at the areas<br />
of mucosal ulceration. There was no evidence of any<br />
other pathology; in particular, there was no evidence<br />
of Crohn’s disease, malignancy or other inflammatory<br />
bowel disease and specific immune-histochemistry<br />
stains were not performed.<br />
DISCUSSION<br />
DD was first described in 1988 [1] as circumferential<br />
mucosal lesions forming “diaphragms” within the<br />
small bowel. The small bowel is most commonly<br />
affected although similar lesions have been reported<br />
in the colon [2] . Histologically, diaphragms are similar<br />
to the normal plicae circulares in the small bowel but<br />
with submucosal fibrosis, and occasional mucosal<br />
ulceration and villous atrophy [1] .<br />
There is a clear association between DD and<br />
long-term NSAID use and NSAIDs are known to<br />
affect enterocytes directly by increasing intestinal<br />
permeability [3] , which might allow bacterial invasion<br />
of the bowel wall with secondary inflammation. DD<br />
in the absence of NSAID use is very rare although<br />
unknown NSAID ingestion was possible in these<br />
cases [2,4] . In this case, given the long term management<br />
of chronic leg pain, formal documentation of<br />
analgesics prescribed both in the community and<br />
hospital settings was available and we are confident<br />
that there was no prior NSAID use. We are unsure as<br />
to the etiology of diaphragm disease in this case and,<br />
on histopathological analysis, there was no chronic<br />
inflammation or ulceration, suggesting that systemic<br />
factors may have a role.<br />
Radiological investigations, as in this case, can<br />
be misleading and can often overlook intra-luminal<br />
diaphragms. The diagnosis is usually confirmed on<br />
histopathological analysis although can be suspected<br />
from other imaging techniques such as capsule<br />
endoscopy, small bowel enteroscopy, small bowel<br />
contrast studies or enteroclysis. The tendency for<br />
objects to be retained within diaphragm compartments<br />
themselves may also be useful for diagnosis [5] .<br />
Progressive obstruction caused by diaphragm<br />
disease requires surgical resection of the affected bowel<br />
and strictuloplasty-type operations are of no benefit<br />
given the circumferential nature of the disease. There<br />
is no current guidance on the management of other<br />
diaphragms found at surgery. In this case, resection<br />
was not possible given the length of bowel that was<br />
affected and as such an intra-operative decision to<br />
leave bowel that had a patent lumen was taken and













