

A Guide to Primary Care of People with HIV/AIDS - Canadian Public ...
A Guide to Primary Care of People with HIV/AIDS - Canadian Public ...
A Guide to Primary Care of People with HIV/AIDS - Canadian Public ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
A <strong>Guide</strong> <strong>to</strong> <strong>Primary</strong> <strong>Care</strong> <strong>of</strong> <strong>People</strong> <strong>with</strong> <strong>HIV</strong>/<strong>AIDS</strong><br />
Chapter 5: Antiretroviral Therapy<br />
How do you decide on a specific regimen?<br />
The selection <strong>of</strong> a regimen is based on the experience<br />
<strong>with</strong> completed trials and idiosyncrasies <strong>of</strong> the specific<br />
patients. No single regimen is appropriate for all<br />
patients, but virtually all experienced <strong>AIDS</strong> treaters have<br />
a few favorites. Most start <strong>with</strong> a 3- or 4-drug regimen<br />
that includes 1) an NNRTI combined <strong>with</strong> 2 nucleosides,<br />
2) a PI either alone or boosted <strong>with</strong> ri<strong>to</strong>navir (RTV)<br />
plus 2 nucleosides, or 3) a 3-nucleoside regimen<br />
that includes abacavir (ABC), lamivudine (3TC), and<br />
zidovudine (combined as Trizivir). This last regimen has<br />
been popular for patients who struggle <strong>with</strong> complicated<br />
medical regimens because it is only 1 pill twice a<br />
day; however, the regimen is considered suboptimal<br />
compared <strong>with</strong> the PI- or NNRTI-based regimens.<br />
Is once-a-day therapy possible?<br />
This is now feasible and clearly preferred by some<br />
patients. The following drugs may be given once a day:<br />
ten<strong>of</strong>ovir (TDF), lamivudine (3TC), emtricitabine (FTC),<br />
didanosine (ddI), stavudine (d4T), efavirenz (EFV),<br />
atazanavir (ATV), and amprenavir plus ri<strong>to</strong>navir (APV/r).<br />
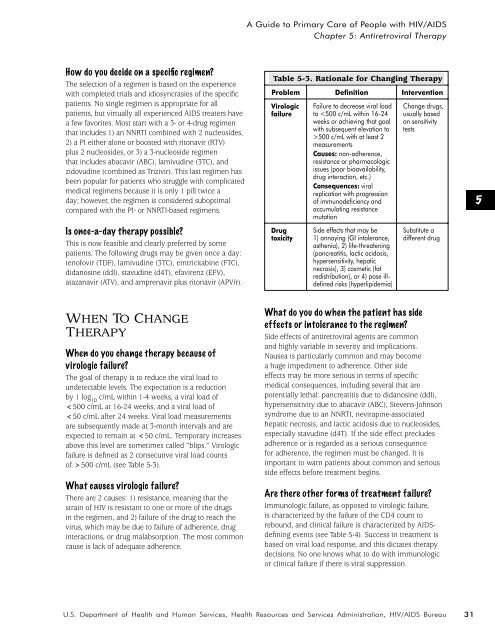
Table 5-3. Rationale for Changing Therapy<br />
Problem Definition Intervention<br />
Virologic<br />
failure<br />
Drug<br />
<strong>to</strong>xicity<br />
Failure <strong>to</strong> decrease viral load<br />
<strong>to</strong> 500 c/mL <strong>with</strong> at least 2<br />
measurements<br />
Causes: non-adherence,<br />
resistance or pharmacologic<br />
issues (poor bioavailability,<br />
drug interaction, etc.)<br />
Consequences: viral<br />
replication <strong>with</strong> progression<br />
<strong>of</strong> immunodeficiency and<br />
accumulating resistance<br />
mutation<br />
Side effects that may be<br />
1) annoying (GI in<strong>to</strong>lerance,<br />
asthenia), 2) life-threatening<br />
(pancreatitis, lactic acidosis,<br />
hypersensitivity, hepatic<br />
necrosis), 3) cosmetic (fat<br />
redistribution), or 4) pose illdefined<br />
risks (hyperlipidemia)<br />
Change drugs,<br />
usually based<br />
on sensitivity<br />
tests<br />
Substitute a<br />
different drug<br />
5<br />
WHEN TO CHANGE<br />
THERAPY<br />
When do you change therapy because <strong>of</strong><br />
virologic failure?<br />
The goal <strong>of</strong> therapy is <strong>to</strong> reduce the viral load <strong>to</strong><br />
undetectable levels. The expectation is a reduction<br />
by 1 log 10<br />
c/mL <strong>with</strong>in 1-4 weeks, a viral load <strong>of</strong><br />














