

A Guide to Primary Care of People with HIV/AIDS - Canadian Public ...
A Guide to Primary Care of People with HIV/AIDS - Canadian Public ...
A Guide to Primary Care of People with HIV/AIDS - Canadian Public ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
A <strong>Guide</strong> <strong>to</strong> <strong>Primary</strong> <strong>Care</strong> <strong>of</strong> <strong>People</strong> <strong>with</strong> <strong>HIV</strong>/<strong>AIDS</strong><br />
Chapter 6: Metabolic Complications <strong>of</strong> Antiretroviral Therapy<br />
6<br />
LIPID ABNORMALITIES<br />
What antiretroviral medications adversely<br />
affect lipid levels?<br />
Available data suggest that drugs in the protease<br />
inhibi<strong>to</strong>r (PI) class have the greatest adverse effect<br />
on triglycerides, <strong>to</strong>tal cholesterol, and low-density<br />
lipoprotein (LDL) cholesterol levels. The mechanism<br />
remains unclear. Among the PIs, ri<strong>to</strong>navir (RTV) and<br />
ri<strong>to</strong>navir-boosted regimens appear <strong>to</strong> have the greatest<br />
impact on triglycerides and <strong>to</strong>tal cholesterol levels.<br />
Because some patients who receive ri<strong>to</strong>navir had no<br />
significant changes whereas others have dramatic<br />
increases, genetic predisposition may play a major role.<br />
The PI atazanavir (ATV) does not significantly affect lipid<br />
levels. The impact <strong>of</strong> nucleoside reverse transcriptase<br />
inhibi<strong>to</strong>rs (NRTIs) and non-nucleoside reverse<br />
transcriptase inhibi<strong>to</strong>rs (NNRTIs) on lipid levels has not<br />
been well defined, but the impact appears much less<br />
than changes associated <strong>with</strong> PIs. In 96-week data from<br />
a trial that compared stavudine (d4T) plus lamivudine<br />
(3TC) plus efavirenz (EFV) <strong>with</strong> ten<strong>of</strong>ovir (TDF) plus<br />
lamivudine plus efavirenz, those patients in the<br />
stavudine arm had significantly higher cholesterol and<br />
triglyceride levels. The NNRTI nevirapine (NVP) has no<br />
adverse affect on lipids, and the changes <strong>with</strong> efavirenz<br />
are variable. Patients receiving PIs should undergo<br />
regular moni<strong>to</strong>ring <strong>of</strong> lipid levels (see Table 6-2).<br />
Do antiretroviral drugs cause an increase in<br />
cardiovascular disease?<br />
Several isolated case reports initially suggested ART<br />
could lead <strong>to</strong> cardiovascular disease, including death<br />
from myocardial infarction, in <strong>HIV</strong>-infected patients.<br />
More recent aggregate data from over 20,000 patients<br />
in cohort studies indicate the risk related <strong>to</strong> ART is<br />
low and substantially lower than the risk <strong>of</strong> smoking<br />
(Friss-Moller, et al, 2003). In addition, in a large study<br />
that involved more than 36,000 veterans, investiga<strong>to</strong>rs<br />
found the benefit <strong>of</strong> these drugs far outweighed the<br />
risks. Because cardiovascular disease may take 10-15<br />
years <strong>to</strong> manifest, investiga<strong>to</strong>rs will need long-term<br />
followup <strong>of</strong> individuals who have received ART <strong>to</strong><br />
determine the long-term impact.<br />
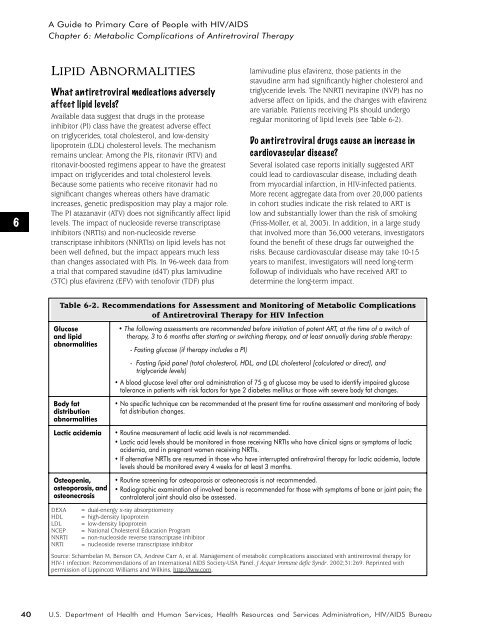
Table 6-2. Recommendations for Assessment and Moni<strong>to</strong>ring <strong>of</strong> Metabolic Complications<br />
<strong>of</strong> Antiretroviral Therapy for <strong>HIV</strong> Infection<br />
Glucose<br />
and lipid<br />
abnormalities<br />
Body fat<br />
distribution<br />
abnormalities<br />
Lactic acidemia<br />
Osteopenia,<br />
osteoporosis, and<br />
osteonecrosis<br />
DEXA<br />
HDL<br />
LDL<br />
NCEP<br />
NNRTI<br />
NRTI<br />
• The following assessments are recommended before initiation <strong>of</strong> potent ART, at the time <strong>of</strong> a switch <strong>of</strong><br />
therapy, 3 <strong>to</strong> 6 months after starting or switching therapy, and at least annually during stable therapy:<br />
- Fasting glucose (if therapy includes a PI)<br />
- Fasting lipid panel (<strong>to</strong>tal cholesterol, HDL, and LDL cholesterol [calculated or direct], and<br />
triglyceride levels)<br />
• A blood glucose level after oral administration <strong>of</strong> 75 g <strong>of</strong> glucose may be used <strong>to</strong> identify impaired glucose<br />
<strong>to</strong>lerance in patients <strong>with</strong> risk fac<strong>to</strong>rs for type 2 diabetes mellitus or those <strong>with</strong> severe body fat changes.<br />
• No specific technique can be recommended at the present time for routine assessment and moni<strong>to</strong>ring <strong>of</strong> body<br />
fat distribution changes.<br />
• Routine measurement <strong>of</strong> lactic acid levels is not recommended.<br />
• Lactic acid levels should be moni<strong>to</strong>red in those receiving NRTIs who have clinical signs or symp<strong>to</strong>ms <strong>of</strong> lactic<br />
acidemia, and in pregnant women receiving NRTIs.<br />
• If alternative NRTIs are resumed in those who have interrupted antiretroviral therapy for lactic acidemia, lactate<br />
levels should be moni<strong>to</strong>red every 4 weeks for at least 3 months.<br />
• Routine screening for osteoporosis or osteonecrosis is not recommended.<br />
• Radiographic examination <strong>of</strong> involved bone is recommended for those <strong>with</strong> symp<strong>to</strong>ms <strong>of</strong> bone or joint pain; the<br />
contralateral joint should also be assessed.<br />
= dual-energy x-ray absorptiometry<br />
= high-density lipoprotein<br />
= low-density lipoprotein<br />
= National Cholesterol Education Program<br />
= non-nucleoside reverse transcriptase inhibi<strong>to</strong>r<br />
= nucleoside reverse transcriptase inhibi<strong>to</strong>r<br />
Source: Schambelan M, Benson CA, Andrew Carr A, et al. Management <strong>of</strong> metabolic complications associated <strong>with</strong> antiretroviral therapy for<br />
<strong>HIV</strong>-1 infection: Recommendations <strong>of</strong> an International <strong>AIDS</strong> Society-USA Panel. J Acquir Immune defic Syndr. 2002;31:269. Reprinted <strong>with</strong><br />
permission <strong>of</strong> Lippincott Williams and Wilkins, http://lww.com.<br />
40<br />
U.S. Department <strong>of</strong> Health and Human Services, Health Resources and Services Administration, <strong>HIV</strong>/<strong>AIDS</strong> Bureau














