

Vol 43 # 2 June 2011 - Kma.org.kw
Vol 43 # 2 June 2011 - Kma.org.kw
Vol 43 # 2 June 2011 - Kma.org.kw

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>June</strong> <strong>2011</strong><br />
KUWAIT MEDICAL JOURNAL 121<br />
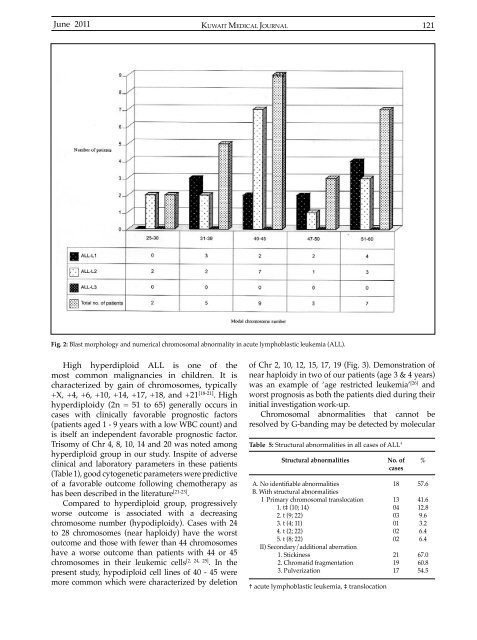
Fig. 2: Blast morphology and numerical chromosomal abnormality in acute lymphoblastic leukemia (ALL).<br />
High hyperdiploid ALL is one of the<br />
most common malignancies in children. It is<br />
characterized by gain of chromosomes, typically<br />
+X, +4, +6, +10, +14, +17, +18, and +21 [18-21] . High<br />
hyperdiploidy (2n = 51 to 65) generally occurs in<br />
cases with clinically favorable prognostic factors<br />
(patients aged 1 - 9 years with a low WBC count) and<br />
is itself an independent favorable prognostic factor.<br />
Trisomy of Chr 4, 8, 10, 14 and 20 was noted among<br />
hyperdiploid group in our study. Inspite of adverse<br />
clinical and laboratory parameters in these patients<br />
(Table 1), good cytogenetic parameters were predictive<br />
of a favorable outcome following chemotherapy as<br />
has been described in the literature [21-23] .<br />
Compared to hyperdiploid group, progressively<br />
worse outcome is associated with a decreasing<br />
chromosome number (hypodiploidy). Cases with 24<br />
to 28 chromosomes (near haploidy) have the worst<br />
outcome and those with fewer than 44 chromosomes<br />
have a worse outcome than patients with 44 or 45<br />
chromosomes in their leukemic cells [2, 24, 25] . In the<br />
present study, hypodiploid cell lines of 40 - 45 were<br />
more common which were characterized by deletion<br />
of Chr 2, 10, 12, 15, 17, 19 (Fig. 3). Demonstration of<br />
near haploidy in two of our patients (age 3 & 4 years)<br />
was an example of ‘age restricted leukemia’ [26] and<br />
worst prognosis as both the patients died during their<br />
initial investigation work-up.<br />
Chromosomal abnormalities that cannot be<br />
resolved by G-banding may be detected by molecular<br />
Table 5: Structural abnormalities in all cases of ALL †<br />
Structural abnormalities<br />
A. No identifiable abnormalities<br />
B. With structural abnormalities<br />
I Primary chromosomal translocation<br />
1. t‡ (10; 14)<br />
2. t (9; 22)<br />
3. t (4; 11)<br />
4. t (2; 22)<br />
5. t (8; 22)<br />
II) Secondary/additional aberration<br />
1. Stickiness<br />
2. Chromatid fragmentation<br />
3. Pulverization<br />
† acute lymphoblastic leukemia, ‡ translocation<br />
No. of<br />
cases<br />
18<br />
13<br />
04<br />
03<br />
01<br />
02<br />
02<br />
21<br />
19<br />
17<br />
%<br />
57.6<br />
41.6<br />
12.8<br />
9.6<br />
3.2<br />
6.4<br />
6.4<br />
67.0<br />
60.8<br />
54.5













